Get Wsi Ffirst Report Of Injury Form
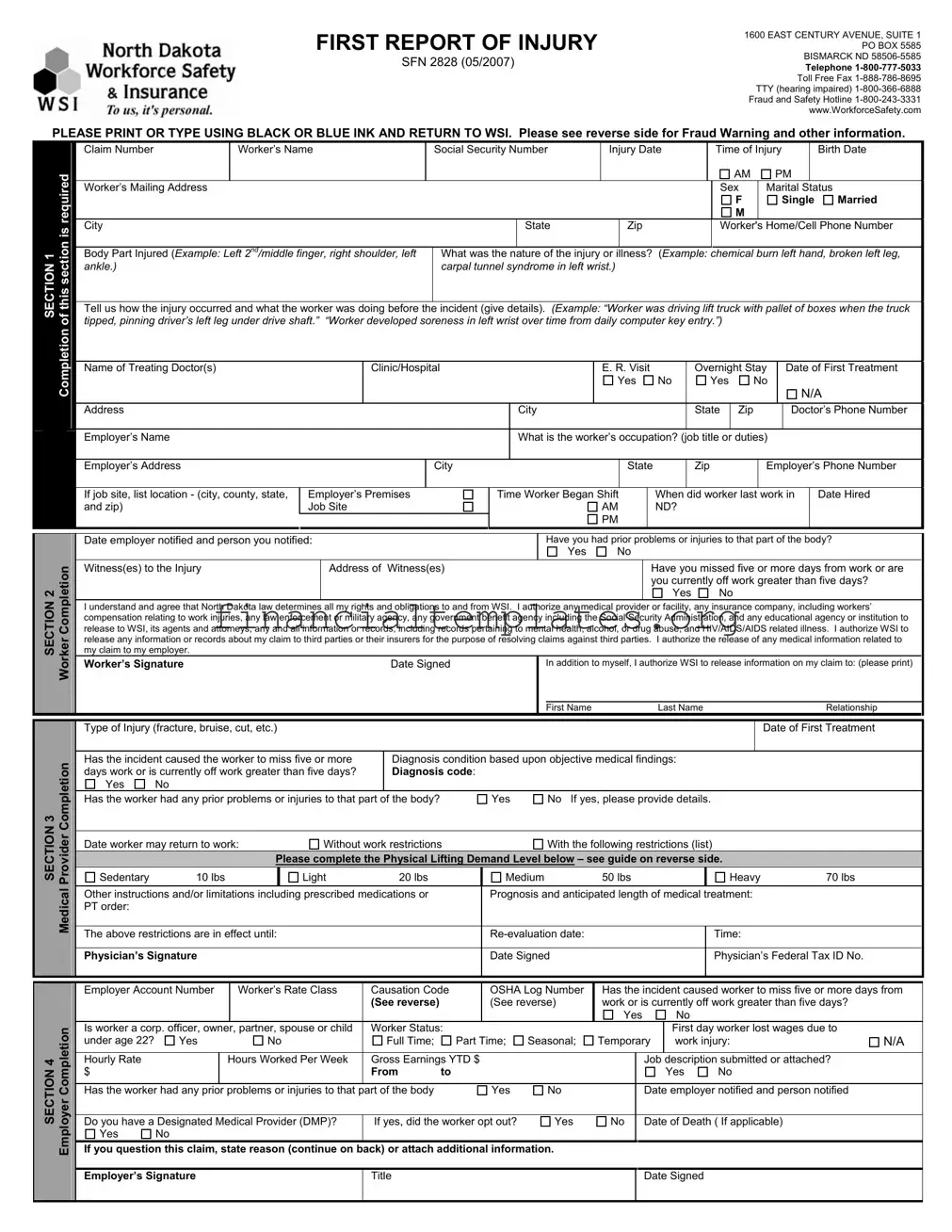
Navigating workplace injuries requires thorough documentation to ensure both the injured worker receives appropriate care and benefits, and that employers comply with regulatory obligations. Key to this process is the First Report of Injury form provided by Workforce Safety & Insurance (WSI) in North Dakota, with its headquarters located at 1600 East Century Avenue, Suite 1, P.O. Box 5585, Bismarck, ND 58506-5585. The form, which should be filled out using black or blue ink, is a comprehensive document designed to capture all relevant information pertaining to a workplace injury. It includes sections for detailed information about the worker (including name, contact information, social security number, and job details), the nature of the injury or illness, how the incident occurred, treatment received, and the physician's diagnosis and prognosis. Furthermore, instructions on the reverse side of the form provide guidance on completing it accurately, which is crucial for processing the claim effectively. Employers also have designated sections to fill, including details about the employment status of the injured worker and whether the worker had any prior injuries to the same body part. The form emphasizes the importance of honesty and accuracy in reporting, with warnings about the consequences of filing false claims. Overall, this document serves as the initial step in navigating the claims process, aiming to streamline the collection of information necessary for the timely and fair resolution of workers' compensation claims.
Wsi Ffirst Report Of Injury Example
FIRST REPORT OF INJURY |
1600 EAST CENTURY AVENUE, SUITE 1 |
|
PO BOX 5585 |
||
SFN 2828 (05/2007) |
BISMARCK ND |
|
Telephone |
||
|
||
|
Toll Free Fax |
|
|
TTY (hearing impaired) |
|
|
Fraud and Safety Hotline |
|
|
www.WorkforceSafety.com |
PLEASE PRINT OR TYPE USING BLACK OR BLUE INK AND RETURN TO WSI. Please see reverse side for Fraud Warning and other information.
SECTION 1
SECTION 2
SECTION 3
|
|
Claim Number |
|
Worker’s Name |
|
|
Social Security Number |
Injury Date |
|
|
Time of Injury |
|
Birth Date |
|
||||||||||||||||||||||
required |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
|
PM |
|
|
|
||||
|
Worker’s Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sex |
|
Marital Status |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
|
|
Single |
Married |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
is |
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
Zip |
|
|
|
|
Worker's Home/Cell Phone Number |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
sectionthis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Body Part Injured (Example: Left 2nd/middle finger, right shoulder, left |
What was the nature of the injury or illness? (Example: chemical burn left hand, broken left leg, |
|
|||||||||||||||||||||||||||||||||
|
|
|
||||||||||||||||||||||||||||||||||
|
|
ankle.) |
|
|
|
|
|
|
|
|
carpal tunnel syndrome in left wrist.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
of |
|
Tell us how the injury occurred and what the worker was doing before the incident (give details). (Example: “Worker was driving lift truck with pallet of boxes when the truck |
|
|||||||||||||||||||||||||||||||||
|
tipped, pinning driver’s left leg under drive shaft.” “Worker developed soreness in left wrist over time from daily computer key entry.”) |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Completion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Treating Doctor(s) |
|
|
Clinic/Hospital |
|
|
|
|
|
|
E. R. Visit |
|
|
Overnight Stay |
|
|
Date of First Treatment |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
Yes |
No |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N/A |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
State |
Zip |
|
|
|
Doctor’s Phone Number |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Employer’s Name |
|
|
|
|
|
|
|
|
|
What is the worker’s occupation? (job title or duties) |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Employer’s Address |
|
|
|
|
|
City |
|
|
|
|
|
|
|
State |
|
|
Zip |
|
|
|
Employer’s Phone Number |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
If job site, list location - (city, county, state, |
Employer’s Premises |
|
|
Time Worker Began Shift |
|
When did worker last work in |
|
Date Hired |
|
|||||||||||||||||||||||||
|
|
and zip) |
|
|
|
Job Site |
|
|
|
|
|
|
|
|
|
|
AM |
|
ND? |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
Date employer notified and person you notified: |
|
|
|
|
|
|
|
|
Have you had prior problems or injuries to that part of the body? |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Completion |
|
Witness(es) to the Injury |
|
Address of |
Witness(es) |
|
|
|
|
|
|
|
|
Have you missed five or more days from work or are |
|
|||||||||||||||||||||
|
release to WSI, its agents and attorneys, any and all information or records, including records pertaining to mental health, alcohol, or drug abuse, and HIV/AIDS/AIDS related illness. I authorize WSI to |
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
you currently off work greater than five days? |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
||||
|
|
I understand and agree that North Dakota law determines all my rights and obligations to and from WSI. I authorize any medical provider or facility, any insurance company, including workers’ |
|
|||||||||||||||||||||||||||||||||
|
|
compensation relating to work injuries, any law enforcement or military agency, any government benefit agency including the Social Security Administration, and any educational agency or institution to |
|
|||||||||||||||||||||||||||||||||
Worker |
|
release any information or records about my claim to third parties or their insurers for the purpose of resolving claims against third parties. I authorize the release of any medical information related to |
|
|||||||||||||||||||||||||||||||||
|
my claim to my employer. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Worker’s Signature |
|
|
|
Date Signed |
|
|
|
|
In addition to myself, I authorize WSI to release information on my claim to: (please print) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
Last Name |
|
|
|
|
|
|
|
|
Relationship |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Type of Injury (fracture, bruise, cut, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of First Treatment |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
Completion |
|
Has the incident caused the worker to miss five or more |
Diagnosis condition based upon objective medical findings: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
days work or is currently off work greater than five days? |
Diagnosis code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Has the worker had any prior problems or injuries to that part of the body? |
Yes |
|
|
No If yes, please provide details. |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date worker may return to work: |
|
Without work restrictions |
|
|
|
|
With the following restrictions (list) |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
Please complete the Physical Lifting Demand Level below – see guide on reverse side. |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
Sedentary |
10 lbs |
|
Light |
20 lbs |
|
|
Medium |
50 lbs |
|
|
|
|
|
Heavy |
|
|
|
|
|
70 lbs |
|
|||||||||||||
Medical |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other instructions and/or limitations including prescribed medications or |
|
|
Prognosis and anticipated length of medical treatment: |
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
PT order: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
The above restrictions are in effect until: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time: |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
Physician’s Signature |
|
|
|
|
|
|
|
Date Signed |
|
|
|
|
|
|
|
Physician’s Federal Tax ID No. |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer Account Number |
|
Worker’s Rate Class |
Causation Code |
|
OSHA Log Number |
Has the incident caused worker to miss five or more days from |
||||||||
|
|
|
|
|
(See reverse) |
|
|
(See reverse) |
work or is currently off work greater than five days? |
|
|||||
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
|
SECTION 4 Employer Completion |
Is worker a corp. officer, owner, partner, spouse or child |
Worker Status: |
|
|
|
|
|
|
First day worker lost wages due to |
|
|||||
under age 22? |
Yes |
|
No |
Full Time; |
|
Part Time; |
Seasonal; |
Temporary |
work injury: |
N/A |
|||||
|
|
|
|
|
|
|
|
|
|
||||||
Hourly Rate |
|
Hours Worked Per Week |
Gross Earnings YTD $ |
|
|
|
Job description submitted or attached? |
|
|||||||
$ |
|
|
|
From |
to |
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Has the worker had any prior problems or injuries to that part of the body |
|
|
Yes |
No |
|
|
Date employer notified and person notified |
|
|||||||
|
|
|
|
|
|
|
|||||||||
Do you have a Designated Medical Provider (DMP)? |
If yes, did the worker opt out? |
Yes |
No |
|
Date of Death ( If applicable) |
|
|||||||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If you question this claim, state reason (continue on back) or attach additional information. |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Employer’s Signature |
|
|
Title |
|
|
|
|
|
|
Date Signed |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Any person claiming benefits or compensation from WSI who files a false claim, or makes a false statement, or fails to notify WSI as to the receipt of income or an increase in income from employment, in connection with any claim or application for workers’ compensation benefits will forfeit any future benefits and may be guilty of a felony which is punishable by imprisonment, substantial fines, or both. These criminal penalties are applicable to all persons dealing with the Fund, including injured workers, employers, medical providers, and attorneys.
To report an instance of fraud, contact the ND Fraud and Safety Hotline at
For medical provider use:
|
Physical Demand Level |
|
Occasional |
|
Frequent |
|
Constant |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sedentary |
|
10 lbs. |
|
Negligible |
|
Negligible |
|
|
|
|
|
|
|
|
|
Light |
|
20 lbs. |
|
10 lbs. and/or Walk/Stand/Push/Pull |
|
Negligible and/or Push/Pull of |
|
|
|
of Arm/Leg controls |
|
Arm/Leg controls while seated. |
||
|
|
|
|
|
|
||
|
Medium |
|
50 lbs. |
|
20 lbs. |
|
10 lbs. |
|
|
|
|
|
|
|
|
|
Heavy |
|
70 lbs. |
|
50 lbs. |
|
20 lbs. |
|
|
|
|
|
|
|
|
For employer use:
Causation Codes:
1.Contact with object and/or equipment
2.Fall to lower level
3.Fall on same level
4.Slip, trip, or loss of balance without fall
5.Overexertion
6.Overexertion lifting
7.Repetitive motion
8.Exposure to harmful substances
9.Transportation accident
10.Fire and/or explosion
11.Assault and/or violent act
For more information regarding the OSHA Log number (OSHA 300 Reference Number), visit
Document Specifics
| Fact | Detail |
|---|---|
| Form Identification | The form is known as the First Report of Injury, with the identifier SFN 2828 (05/2007). |
| Location Details | The form is issued from 1600 East Century Avenue, Suite 1, PO Box 5585, Bismarck, ND 58506-5585. |
| Contact Information | Telephone contact is available at 1-800-777-5033, with a toll-free fax at 1-888-786-8695 and TTY (for the hearing impaired) at 1-800-366-6888. |
| Fraud and Safety Hotline | A specific hotline for reporting fraud and safety concerns is provided at 1-800-243-3331. |
| Governing Law | The worker authorizes that North Dakota law will determine all rights and obligations related to the Workforce Safety & Insurance (WSI). |
Guide to Writing Wsi Ffirst Report Of Injury
Filling out the First Report of Injury form is a critical step in initiating the workers' compensation claims process. This form ensures that an incident is officially recorded and sets the foundation for any potential claims. It's important to provide accurate and detailed information to facilitate a smooth evaluation and decision regarding the claim. Here's how to correctly fill out this form:
- Section 1: Enter the worker's details including their name, Social Security Number, date of birth, gender, marital status, contact information, and mailing address.
- Section 2: Detail the injury or illness, specifying the exact body part affected and the nature of the injury. Describe how the incident occurred, including what the worker was doing at the time, ensuring to provide comprehensive details.
- In the same section, input the name, address, and phone number of the treating doctor(s) alongside the clinic or hospital details. If there was an emergency room visit or an overnight stay in the hospital, indicate this by ticking 'Yes' or 'No'.
- Provide the worker's occupation, including job title or duties, employer's name, address, phone number, and location of the job site if applicable. Mention the date and time the worker started their shift, the last date the worker worked, and the date and person who was notified about the injury.
- Answer questions regarding prior problems or injuries to the same body part, witness(es) to the injury, and if the incident has led to the worker missing more than five days of work.
- Section 3: Include any relevant information regarding the type of injury, first date of treatment, if the incident caused the worker to miss more than five days of work, prior issues with the same body part, and the doctor’s diagnosis. Also, specify details regarding the worker’s capacity to return to work, limitations, treatment prognosis, and lifting limitations.
- At the end of the section, the worker must sign and date the form, authorizing the release of information necessary for processing the claim.
- Section 4: The employer completes this section, providing information about the worker's employment status, earnings, job description, and if there were previous injuries reported. If the employer questions the claim, they must state their reasons here.
- Lastly, the employer signs and dates the form, certifying the information provided.
Once the form is accurately filled out, it should be submitted using the provided contact details for Workforce Safety & Insurance (WSI). This submission initiates the evaluation process for the worker's compensation claim. Accurate and timely reporting is crucial for a smooth claims process, potentially leading to quicker resolution and support for the injured worker.
Understanding Wsi Ffirst Report Of Injury
FAQ Section: WSI First Report of Injury Form
What is the purpose of the WSI First Report of Injury form?
The form is designed to report workplace injuries to Workforce Safety & Insurance (WSI) in North Dakota. It ensures timely communication of injury details to WSI, facilitating the start of any workers’ compensation claim process. This includes recording the specifics of the injury, diagnosis, and any immediate treatment received.
Who needs to fill out the WSI First Report of Injury form?
The injured worker is responsible for reporting the injury, but the employer also plays a significant role in completing and submitting the form to WSI. Medical providers may need to provide specific details related to the diagnosis and treatment of the injury.
When should the WSI First Report of Injury form be submitted?
It should be submitted to WSI as soon as possible after the injury occurs. Prompt submission can aid in the efficient processing of workers' compensation benefits that the injured employee may be entitled to.
How can the form be submitted to WSI?
The form can be submitted via toll-free fax or mail to the addresses listed at the top of the form. Employers may also have the ability to submit this information online through the WSI portal, if available.
What information is required on the WSI First Report of Injury form?
- Details of the injured worker, including name, contact information, and social security number.
- Specifics of the injury or illness, including how it occurred and the body part affected.
- Information on the treatment received, including the name of the treating doctor, and whether an emergency room visit or overnight hospital stay was required.
- Employment details at the time of injury, including job title, location, and if there were any witnesses.
- Signature of the worker, consenting to the release of information relevant to the claim.
What happens after the form is submitted?
WSI will review the submitted form and begin the process for evaluating the claim. This may involve contacting the injured worker, employer, or medical provider for additional details. The claimant may be assigned a case manager to assist them through the process.
Is there a deadline for filing a claim with WSI after an injury?
Yes, there are deadlines for filing a claim, which can vary depending on the nature of the injury or illness. It's important for workers to report their injury to their employer and fill out the WSI form promptly to avoid delays in receiving potential benefits.
Where can one find more information or assistance with the WSI First Report of Injury form?
Additional information and assistance can be obtained by contacting WSI directly via their toll-free telephone line or by visiting their website. Employers may also provide assistance and resources to help with completing and submitting the form.
Common mistakes
Not using black or blue ink: The form specifically requires that it be filled out using black or blue ink. Using other colors can make the information difficult to read or even result in the form being rejected.
Skipping sections: Every section and question is designed to collect vital information. When people leave out information, it can delay the process or affect the outcome of the claim.
Incomplete or vague descriptions of the injury: It's important to be as specific as possible about the nature and cause of the injury. Vague descriptions can lead to misunderstandings about the severity and cause of the injury.
Forgetting to list witnesses: If there were any witnesses to the injury, their information could be crucial. Failing to provide this can weaken the claim.
Not reporting prior problems or injuries to the body part: If the worker has had previous issues with the same body part, not disclosing this information could be seen as misleading.
Incorrect or missing employment information: The employer’s details, including address, phone number, and job site location are essential for proper processing of the form.
Omitting doctor’s or treatment details: The name of the treating doctor(s), their phone number, the clinic or hospital visited, dates of visits, and information on whether it was an emergency visit or an overnight stay are critical for a comprehensive understanding of the injury and subsequent care.
Avoiding these mistakes helps ensure the form is correctly processed, facilitating a smoother and quicker claim resolution:
- Use only black or blue ink: This ensures the form is legible and meets submission criteria.
- Complete all sections: Do not leave any section blank. If a section does not apply, note it as "N/A" or "Not Applicable."
- Provide detailed descriptions: Give a clear and precise account of the injury and how it occurred.
- Include witness information: If available, provide names and contact details.
- Disclose prior injuries: Being transparent about previous issues can prevent misunderstandings later on.
- Fill in all employment and medical provider information accurately: This ensures all necessary parties are informed and involved in the claims process.
- Remember to sign and date the form: A signature is required to process the form and claim.
Documents used along the form
When handling a workers' compensation claim, the First Report of Injury form is a crucial starting point. However, to navigate the complexities of such claims efficiently, several other forms and documents often play vital roles throughout the process. Each has its unique function, serving to provide comprehensive detail, ensure compliance, and facilitate the timely and accurate processing of a claim.
- Employee's Claim for Workers' Compensation Benefits (DWC 1): This form is filled out by the employee to officially file a claim for workers’ compensation benefits with their employer.
- Employer’s Report of Occupational Injury or Illness: Employers use this document to report an employee's work-related injury or illness to their workers' compensation insurance carrier.
- Wage Statement (Employer): This document, provided by the employer, outlines the injured worker's earnings, which is crucial for determining benefit amounts.
- Medical Provider Network (MPN) Notification: This form is used in states with MPN systems to inform an injured worker about the network of approved healthcare providers from which they can seek treatment.
- Workers’ Compensation Medical Authorization Form: This form grants permission for the release of medical information to the employer or insurance carrier, facilitating the evaluation of the injury claim.
- Permanent and Stationary Report: A physician's report declaring when an injury has stabilized and is not expected to improve significantly. This report helps in determining the degree of permanent disability.
- Request for Authorization (RFA): Healthcare providers use this form to request authorization from the insurance carrier to provide specific treatments or diagnostic tests to the injured worker.
- Notice of Temporary Disability (NTD): If an injured worker is temporarily unable to work due to their injury, this notice helps to initiate temporary disability payments.
- Return to Work (RTW) Form: This document is utilized once an injured worker is ready to return to work, either in their regular role or in a modified/alternative capacity, detailing any work restrictions.
- Compromise and Release Agreement: This legal document, often used to settle a workers’ compensation claim, outlines an agreed-upon settlement amount to be paid to the injured worker in exchange for closing the claim.
Understanding and utilizing these documents efficiently is fundamental to administering workers' compensation claims. Each form ensures that the process is managed transparently and systematically, safeguarding the interests of all parties involved: the injured worker, the employer, and the insurance carrier. Streamlining this process not only expedites the delivery of benefits to injured workers but also helps in maintaining compliance with state workers' compensation laws and regulations.
Similar forms
The Workers' Compensation Claim Form shares several similarities with the First Report of Injury form, primarily serving as the initial document to report a workplace injury or illness. Like the First Report of Injury, it collects detailed information about the incident, including the injured worker's personal information, the circumstances leading to the injury, and the immediate medical response. Both forms are crucial for initiating the claims process and ensuring that the worker receives appropriate medical attention and compensation benefits in a timely manner.
The Occupational Safety and Health Administration (OSHA) 300 Log is another document that mirrors the First Report of Injury in terms of content. This form requires detailed recording of work-related injuries and illnesses, focusing on the specifics of each incident to help improve workplace safety and health standards. Unlike the First Report of Injury, which is used to file a claim, the OSHA 300 Log's purpose is to track injury trends over time, aiding in the identification and mitigation of workplace hazards.
Disability Insurance Claim Forms also bear resemblance to the First Report of Injury form. These documents are used when an employee is unable to work due to a disability and needs to claim benefits. Similar information is gathered about the nature of the injury or illness, treatment received, and expected duration of the disability. However, these forms are specifically for insurance claims outside of the workers' compensation system, focusing on income replacement for disabilities not necessarily caused by workplace incidents.
The Medical Release Form, while not a report of injury per se, complements the First Report of Injury form by authorizing the release and exchange of medical information between healthcare providers and insurance carriers. This form ensures that relevant medical records can be accessed to authenticate the injury details provided in the First Report of Injury, facilitating the claims process and ensuring that decisions are based on accurate medical data.
Incident Report Forms, used by businesses to document any unusual or unexpected occurrences that are not necessarily related to injuries, can also be likened to the First Report of Injury form. These documents capture the specifics of an incident, including date, time, and description, to assist in future investigations or to implement preventive measures. Though broader in scope, they serve a similar purpose in record-keeping and potential legal protection for the organization.
Return to Work Forms partially overlap with the First Report of Injury form in their use within the context of an injury or illness. These forms focus on the worker's readiness to resume work, outlining any temporary or permanent work restrictions based on medical advice. This is a step that comes later in the process, following an initial report of injury, but is crucial for managing the worker's safe and effective reintegration into the workplace.
Finally, the Auto Accident Personal Injury Claim Form shares similarities with the First Report of Injury form in the context of documenting injuries. Although one pertains to workplace injuries and the other to vehicular accidents, both require detailed accounts of how the injuries occurred, the nature and extent of those injuries, and the initial medical response. These forms are critical in the claims process for insurance purposes, ensuring that all relevant details are captured accurately for record-keeping and dispute resolution.
Dos and Don'ts
When filling out the First Report of Injury form, there are several do's and don'ts to keep in mind to ensure that your form is both accurate and complete. Here's a quick guide to help you through the process:
Do's:- Use black or blue ink to ensure the form is legible and scans correctly.
- Ensure all information is printed clearly, avoiding any handwriting that may be difficult to read.
- Provide detailed descriptions of the injury, including how it occurred and the specific body part affected.
- Include the correct dates and times related to the injury and any medical treatment received.
- Make sure to sign and date the form, as this is a critical requirement for the form's validity.
- Check that you've filled out every required section before submitting the form.
- Do not leave sections blank; if a section does not apply, indicate with "N/A" to show it was not overlooked.
- Avoid using any kind of markers or highlighters, as they might make the form hard to read or scan.
- Do not guess on details; if you're unsure about certain information, take the time to verify it before completing the form.
- Refrain from providing unnecessary personal information about the worker, such as details not relevant to the injury or claim.
- Do not submit the form without reviewing it for accuracy and completeness.
- Avoid waiting too long to submit the form; timely submission is important to ensure the claim can be processed as soon as possible.
Remembering these simple guidelines will help streamline the process of filing an injury report, ensuring that it is done correctly and efficiently.
Misconceptions
There are numerous misconceptions about the First Report of Injury form used by Workforce Safety & Insurance (WSI) in North Dakota. Understanding these can help ensure accurate and prompt reporting of workplace injuries.
Misconception 1: Only serious injuries need to be reported. All workplace injuries, regardless of severity, should be reported to WSI to ensure that the worker receives the necessary support and to comply with state requirements.
Misconception 2: The form is too complicated and requires legal expertise to complete. While detailed, the form is designed to be filled out without legal expertise. Instructions are provided to guide employers and employees through the process.
Misconception 3: Reporting an injury will automatically lead to increased insurance premiums for the employer. Insurance premiums are influenced by numerous factors, and a single claim does not necessarily lead to an increase.
Misconception 4: Personal health information disclosed during the claim process is not protected. All personal health information is handled in compliance with privacy laws and is used strictly for the purpose of processing the claim.
Misconception 5: Only the employer can fill out the form. Either the employer or the injured worker can initiate the process. However, both parties need to provide necessary information.
Misconception 6: If an employee waits too long to report an injury, they lose their rights to benefits. Employees should report injuries as soon as possible, but there are provisions for late reporting under certain circumstances.
Misconception 7: The First Report of Injury form is the only step required to claim benefits. Submitting this form is just the first step. The WSI may require additional information or documentation during the claims process.
Clearing up these misconceptions is crucial for ensuring that all workplace injuries are reported accurately and efficiently, helping both employees and employers navigate the claims process with greater confidence.
Key takeaways
Filing a First Report of Injury form is a critical step in the claims process for workers' compensation. It serves as the initial notification and documentation of an injury or illness that occurs at the workplace or as a result of employment. Here are four key takeaways about filling out and using this form:
- It's essential to use black or blue ink and ensure that all information is printed or typed clearly to avoid any delays in processing the claim.
- The form requires detailed information about the injury or illness, including the body part affected, nature of the injury or illness, how the injury occurred, and any witnesses. Providing complete and accurate details helps in assessing the claim efficiently.
- Timeliness is crucial; the form must be submitted to the appropriate office as soon as possible after the injury occurs. Early reporting can lead to a smoother and faster claim process.
- Fraud warnings are included on the form to remind all parties involved in the claim process that submitting false information can result in severe penalties, including forfeiture of benefits and criminal charges.
Moreover, the inclusion of specific sections for both the worker and the employer ensures that comprehensive information is gathered from both perspectives. This thorough approach aids in evaluating the extent of the injury and determining the appropriate compensation and support needed by the injured worker.
Popular PDF Documents
Pay Sales Tax Colorado - Get your Denver business up and running by completing the Denver Sales, Use, Lodger's Tax License, and Occupational Tax Registration form today.
IRS 990-EZ - The IRS 990-EZ form is a simplified tax document for small to medium-sized tax-exempt organizations, reporting their financial activities.
What Is a Pay Off Letter - Choose how you receive your mortgage payoff details with options provided in our form.