Get Tennessee First Report Form
In the state of Tennessee, the Employer’s First Report of Work Injury or Illness serves as a critical document under the Tennessee Workers' Compensation Law. This mandatory form, outlined by the Tennessee Department of Labor and Workforce Development, is an essential step in the process following a workplace injury or illness, requiring prompt completion and filing with the employer's insurance carrier. The form includes comprehensive sections covering a vast array of data points from the jurisdiction claim number, claim type, and detailed employer and insurance carrier information, to the specifics of the injured or ill employee's situation—such as employment status, nature of the injury or illness, and how the event occurred. It also deals sternly with fraud, marking it as a criminal offense to submit false, incomplete, or misleading information, an act punishable by imprisonment, fines, and denial of insurance benefits. Moreover, the state provides a Benefit Review System, featuring workers' compensation specialists to assist and answer inquiries, emphasizing the form's role in not just documenting but facilitating the claims process. A clear understanding of this form not only aids in maintaining legal compliance but also in supporting affected employees through their recovery and claims process, reinforcing the broader objective of workplace safety and employee welfare in Tennessee.
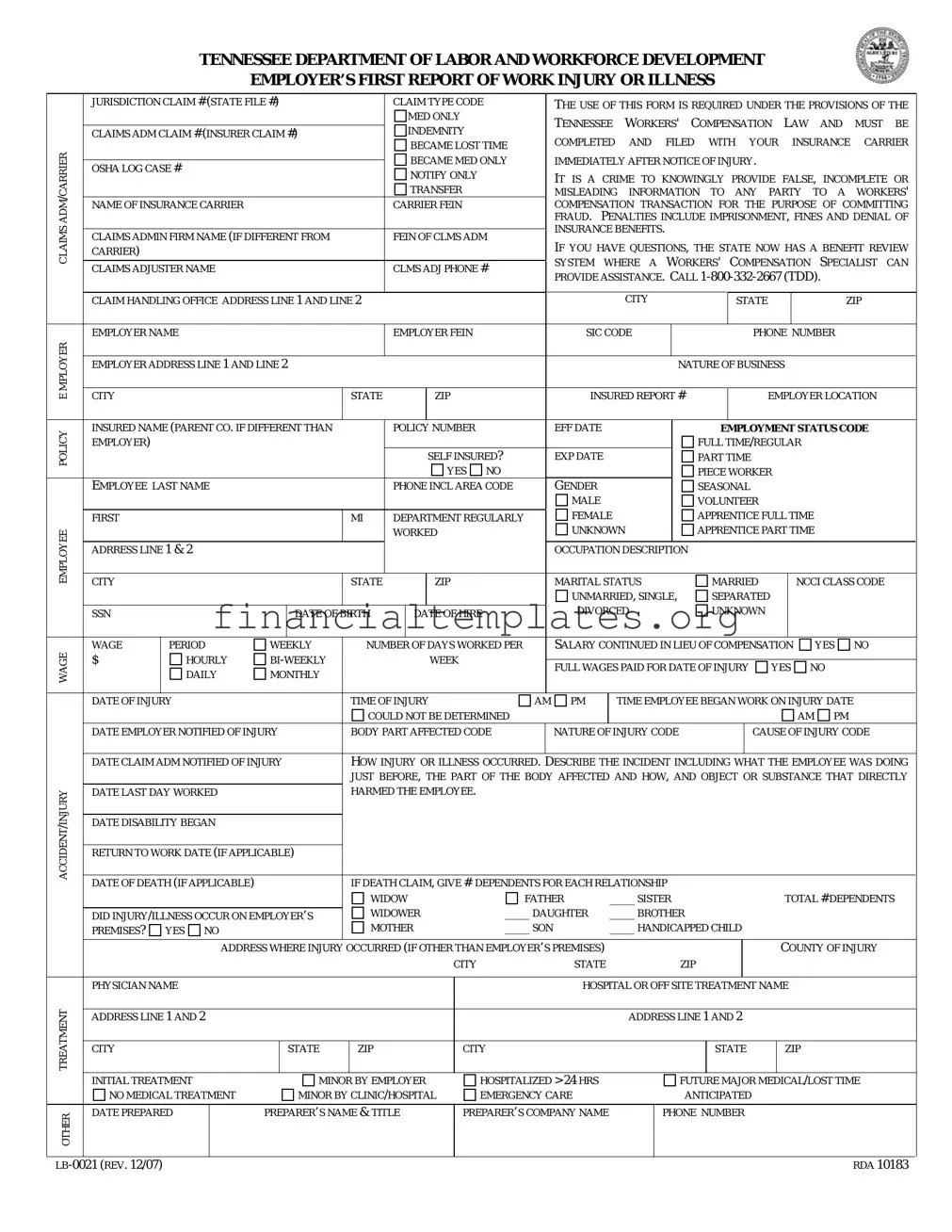
Tennessee First Report Example
TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT
EMPLOYER’S FIRST REPORT OF WORK INJURY OR ILLNESS
|
JURISDICTION CLAIM # (STATE FILE #) |
|
|
|
CLAIM TYPE CODE |
|
THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
MED ONLY |
|
|
TENNESSEE |
WORKERS' |
|
COMPENSATION |
LAW |
AND |
MUST |
BE |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
INDEMNITY |
|
|
|
|||||||||||||||||||||
|
CLAIMS ADM CLAIM # (INSURER CLAIM #) |
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
COMPLETED |
AND |
FILED WITH |
YOUR |
|
|
INSURANCE |
CARRIER |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME LOST TIME |
|
|
|
|||||||||||||||||||||
CARRIER |
|
|
|
|
|
|
|
|
|
|
|
|
IT IS A CRIME TO KNOWINGLY PROVIDE FALSE, INCOMPLETE OR |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
TRANSFER |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
BECAME MED ONLY |
|
IMMEDIATELY AFTER NOTICE OF INJURY. |
|
|
|
|
|
|
||||||||||||||||
|
OSHA LOG CASE # |
|
|
|
|
|
|
|
NOTIFY ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MISLEADING INFORMATION TO ANY PARTY TO A WORKERS' |
|||||||||||||||||||
ADM |
NAME OF INSURANCE CARRIER |
|
|
|
|
|
|
CARRIER FEIN |
|
|
COMPENSATION TRANSACTION FOR THE PURPOSE OF COMMITTING |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FRAUD. |
PENALTIES INCLUDE IMPRISONMENT, FINES AND DENIAL OF |
|||||||||||||||||||
CLAIMS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSURANCE BENEFITS. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CLAIMS ADMIN FIRM NAME (IF DIFFERENT FROM |
|
|
|
FEIN OF CLMS ADM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
IF YOU HAVE QUESTIONS, THE STATE NOW HAS A BENEFIT REVIEW |
||||||||||||||||||||||||||||||||
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
CARRIER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SYSTEM |
WHERE A |
WORKERS' COMPENSATION |
SPECIALIST |
CAN |
|||||||||||||||
|
CLAIMS ADJUSTER NAME |
|
|
|
|
|
|
CLMS ADJ PHONE # |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
PROVIDE ASSISTANCE. CALL |
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CLAIM HANDLING OFFICE ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
ZIP |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
EMPLOYER NAME |
|
|
|
|
|
|
EMPLOYER FEIN |
|
|
SIC CODE |
|
|
|
|
|
|
|
PHONE NUMBER |
|
|
|||||||||||||||
MPLOYERE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
INSURED REPORT # |
EMPLOYER LOCATION |
|
|||||||||||||||||||||||
|
EMPLOYER ADDRESS LINE 1 AND LINE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NATURE OF BUSINESS |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
POLICY |
INSURED NAME (PARENT CO. IF DIFFERENT THAN |
|
|
|
POLICY NUMBER |
|
EFF DATE |
|
|
|
|
|
|
EMPLOYMENT STATUS CODE |
|
|||||||||||||||||||||
EMPLOYER) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FULL TIME/REGULAR |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF INSURED? |
|
EXP DATE |
|
|
|
|
|
PART TIME |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
GENDER |
|
|
|
|
|
|
|
PIECE WORKER |
|
|
|
|
|
|
||||||
|
EMPLOYEE LAST NAME |
|
|
|
|
|
|
PHONE INCL AREA CODE |
|
|
|
|
|
|
|
|
SEASONAL |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MALE |
|
|
|
|
|
|
|
VOLUNTEER |
|
|
|
|
|
|
|||||
|
FIRST |
|
|
|
|
|
|
MI |
|
DEPARTMENT REGULARLY |
|
FEMALE |
|
|
|
|
|
APPRENTICE FULL TIME |
|
|
|
|||||||||||||||
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
WORKED |
|
|
UNKNOWN |
|
|
|
APPRENTICE PART TIME |
|
|
|
|||||||||||||||
ADRRESS LINE 1 & 2 |
|
|
|
|
|
|
|
|
|
|
|
|
OCCUPATION DESCRIPTION |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
CITY |
|
|
|
|
|
|
STATE |
ZIP |
|
|
MARITAL STATUS |
|
|
|
|
MARRIED |
|
|
NCCI CLASS CODE |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNMARRIED, SINGLE, |
|
|
SEPARATED |
|
|
|
|
|
|
||||||||||
|
SSN |
|
|
|
|
DATE OF BIRTH |
|
|
DATE OF HIRE |
|
DIVORCED |
|
|
|
|
UNKNOWN |
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
WAGE |
WAGE |
|
PERIOD |
WEEKLY |
|
NUMBER OF DAYS WORKED PER |
|
SALARY CONTINUED IN LIEU OF COMPENSATION |
|
YES |
NO |
|
||||||||||||||||||||||||
$ |
|
HOURLY |
|
|
|
|
|
WEEK |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
FULL WAGES PAID FOR DATE OF INJURY |
YES NO |
|
|
||||||||||||||||||||||||
|
|
|
DAILY |
MONTHLY |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
DATE OF INJURY |
|
|
|
|
TIME OF INJURY |
|
AM PM |
|
|
TIME EMPLOYEE BEGAN WORK ON INJURY DATE |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
COULD NOT BE DETERMINED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
|
|
||||||
|
DATE EMPLOYER NOTIFIED OF INJURY |
|
BODY PART AFFECTED CODE |
|
NATURE OF INJURY CODE |
|
|
|
|
|
CAUSE OF INJURY CODE |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
DATE CLAIM ADM NOTIFIED OF INJURY |
|
HOW INJURY OR ILLNESS OCCURRED. |
DESCRIBE THE INCIDENT INCLUDING WHAT THE EMPLOYEE WAS DOING |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
JUST BEFORE, THE PART OF THE BODY AFFECTED AND HOW, AND OBJECT OR SUBSTANCE THAT DIRECTLY |
|||||||||||||||||||||||||||
INJURY |
DATE LAST DAY WORKED |
|
|
|
|
HARMED THE EMPLOYEE. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DISABILITY BEGAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ACCIDENT/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RETURN TO WORK DATE (IF APPLICABLE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
IF DEATH CLAIM, GIVE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
DATE OF DEATH (IF APPLICABLE) |
|
|
|
DEPENDENTS FOR EACH RELATIONSHIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
WIDOW |
|
|
|
FATHER |
|
____ SISTER |
|
|
|
|
|
|
|
TOTAL # DEPENDENTS |
||||||||||||
|
|
|
|
|
|
WIDOWER |
|
|
____ DAUGHTER |
|
____ BROTHER |
|
|
|
|
|
|
|
|
|||||||||||||||||
|
DID INJURY/ILLNESS OCCUR ON EMPLOYER’S |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
PREMISES? |
YES NO |
|
|
|
|
|
MOTHER |
|
|
____ SON |
|
____ HANDICAPPED CHILD |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
ADDRESS WHERE INJURY |
OCCURRED (IF OTHER THAN EMPLOYER’S PREMISES) |
|
|
|
|
|
|
|
|
|
|
|
COUNTY OF INJURY |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
|
|
|
|
ZIP |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PHYSICIAN NAME |
|
|
|
|
|
|
|
|
|
|
|
|
HOSPITAL OR OFF SITE TREATMENT NAME |
|
|
|
|||||||||||||||||||
TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS LINE 1 AND 2 |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
CITY |
|
|
|
|
STATE |
|
ZIP |
|
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
INITIAL TREATMENT |
|
|
MINOR BY EMPLOYER |
|
|
HOSPITALIZED > 24 HRS |
|
|
|
|
|
|
FUTURE MAJOR MEDICAL/LOST TIME |
|
|||||||||||||||||||||
|
NO MEDICAL TREATMENT |
|
|
MINOR BY CLINIC/HOSPITAL |
EMERGENCY CARE |
|
|
|
|
|
|
ANTICIPATED |
|
|
|
|
|
|
||||||||||||||||||
OTHER |
DATE PREPARED |
|
PREPARER’S NAME & TITLE |
|
PREPARER’S COMPANY NAME |
|
|
PHONE NUMBER |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RDA 10183 |
||||
Document Specifics
| Fact Name | Description |
|---|---|
| Governing Law | The use of the Tennessee First Report of Work Injury or Illness form is required under the Tennessee Workers' Compensation Law. |
| Fraud Warning | It is considered a crime to knowingly provide false, incomplete, or misleading information to any party in a workers' compensation transaction for the purpose of committing fraud. Penalties include imprisonment, fines, and denial of insurance benefits. |
| Reporting Requirement | This form must be completed and filed with your insurance carrier immediately after notice of injury. |
| Benefit Review System | If you have questions, the state has a Benefit Review System where a workers' compensation specialist can provide assistance. You can call 1-800-332-2667 (TDD). |
| Information Required | Information required includes employer and insurance carrier details, nature of business, employee information, details of the injury or illness, how the injury occurred, and initial treatment information. |
| Claim Type Classification | The form distinguishes between Medical Only and Indemnity Claims, and accommodates for different scenarios like Transfer Became Med Only or Immediately Notify Only. |
| Initial Treatment Options | The form captures information regarding the initial treatment provided, including options like minor by employer, hospitalization over 24 hours, emergency care, and future major medical/lost time anticipated. |
| Injury/Illness Details | Detailed information about the incident leading to the injury or illness is required, including the specifics of what the employee was doing, the body part affected, and the cause of the injury. |
| Death and Dependents | If applicable, the form requires information on the date of death and the number of dependents, specifying their relationship to the deceased. |
Guide to Writing Tennessee First Report
When a workplace injury or illness occurs in Tennessee, employers have a legal obligation under the Tennessee Workers' Compensation Law to swiftly and accurately report the incident. This not only helps in administering benefits to the afflicted employee but also ensures compliance with state mandates. Providing false or misleading information can result in severe penalties, underlining the significance of filling out the Tennessee First Report of Work Injury or Illness with utmost accuracy. Here is a step-by-step guide for completing this crucial document:
- Begin with the top section by entering the JURISDICTION CLAIM # (STATE FILE #) and the CLAIM TYPE CODE, which categorizes the claim as Medical Only, Indemnity Claims, or others as specified.
- Provide the ADM CLAIM # (INSURER CLAIM #), which is the identification number issued by your insurance carrier for this specific injury or illness report.
- Fill in the section for the NAME OF INSURANCE CARRIER including the CARRIER FEIN (Federal Employer Identification Number) and the CLAIMS ADMIN FIRM NAME if different from the carrier’s name.
- List the CLAIMS ADJUSTER NAME and CLMS ADJ PHONE #, ensuring contact details are accurate to facilitate smooth communication.
- Document the CLAIM HANDLING OFFICE ADDRESS including the city, state, and ZIP code to help identify the right office handling the claim.
- Enter the EMPLOYER NAME, EMPLOYER FEIN, and the specific SIC CODE that relates to the employer's nature of business.
- Detail the EMPLOYER CONTACT INFORMATION, including phone number and full address with city, state, and ZIP.
- Specify the INSURED REPORT # and the POLICY NUMBER along with the policy’s effective and expiration dates.
- For the employee, provide the full name, including the Last Name and First Name, MI (Middle Initial), and other required personal information like date of birth, gender, marital status, SSN, and contact details.
- Describe the employee’s job by including the OCCUPATION DESCRIPTION, NCCI CLASS CODE, and employment status (e.g., full-time, part-time).
- Record details of the injury or illness, including DATE OF INJURY, TIME OF INJURY, how the employer was notified, and a detailed account of how the incident occurred.
- Provide information on where and when the injury was treated, including physician name, hospital details, and the initial treatment administered.
- Complete the form by adding DATE PREPARED, PREPARER’S NAME & TITLE, and PREPARER’S COMPANY NAME along with a contact phone number.
The accurate completion of the Tennessee First Report form is a fundamental step in ensuring that employees receive the appropriate medical care and compensation benefits after a work-related injury or illness. It also serves as an essential record for both insurance carriers and state regulatory bodies to monitor and manage workplace safety and health standards. Following the steps listed above will help employers fulfill their reporting obligations efficiently and compliantly.
Understanding Tennessee First Report
Here's a helpful guide covering the essentials about the Tennessee First Report of Work Injury or Illness form, designed to aid both employers and employees in understanding their responsibilities and the process following a workplace incident.
- What is the Tennessee First Report of Work Injury or Illness Form?
The Tennessee First Report of Work Injury or Illness Form, formally known as form LB-0021, is a document required by the Tennessee Department of Labor and Workforce Development. It serves as the initial notification of an injury or illness that occurs in the workplace, capturing detailed information about the incident, the party involved, and the initial treatment provided.
- When must the form be filed?
It’s crucial to file this form immediately after an employer is notified of a work-related injury or illness. Swift reporting ensures compliance with Tennessee Workers' Compensation Law and facilitates the timely provision of benefits to the injured or ill employee.
- Who is responsible for completing the form?
The employer, upon learning about an employee's work-related injury or illness, is responsible for filling out the form. It’s important for employers to provide complete and accurate information to avoid penalties associated with fraudulent claims.
- How is the form submitted?
Once completed, the form should be submitted to the employer’s insurance carrier. The insurance carrier then processes the claim and takes the necessary steps to address the injury or illness reported.
- What information is required on the form?
The form requires comprehensive details including the employer's name, location, and nature of the business; the employee's personal information, employment status, and description of the injury or illness; and information about the treatment provided immediately after the incident.
- Is this form required for all types of injuries or illnesses?
Yes, the Tennessee First Report of Work Injury or Illness Form must be filed for all injuries and illnesses that arise as a direct result of the employee’s job, regardless of the severity. This ensures that all incidents are documented and can be reviewed if complications arise later.
- What are the penalties for not filing the form?
Failing to file the form can result in severe punishments including fines, imprisonment, and the denial of insurance benefits for the injured or ill employee. It's considered a criminal offense to knowingly provide false information or to withhold information related to a workers’ compensation claim.
- Can the form be filed electronically?
For detailed guidance on electronic submissions, employers should consult with their insurance carrier or the Tennessee Department of Labor and Workforce Development. As procedures may vary, it’s essential to follow the specific instructions provided by these entities.
- What if an employer is self-insured?
Self-insured employers must also complete and submit the LB-0021 form in the event of a workplace injury or illness. The process for filing the claim, however, may differ slightly. Self-insured employers typically work directly with claims administrators or workers' compensation specialists for these purposes.
- Where can employers or employees get assistance if they have questions?
For assistance with the form or related procedures, employers and employees can contact the Tennessee Department of Labor and Workforce Development. They offer a Benefit Review System where a workers' compensation specialist can provide needed guidance. The contact number is 1-800-332-2667.
This guide aims to simplify the steps and clarify the purpose of the Tennessee First Report of Work Injury or Illness form. Remember, maintaining accurate records and promptly reporting incidents is not only a legal obligation but also a crucial aspect of workplace safety and employee well-being.
Common mistakes
When completing the Tennessee First Report of Work Injury or Illness form, it's crucial to provide accurate and complete information to avoid potential repercussions, including claim denial. However, mistakes can happen. Here are eight common errors to watch out for:
- Failing to report the injury immediately after notice. Delays can complicate the processing and investigation of the claim.
- Providing false, incomplete, or misleading information. Not only does this jeopardize the integrity of the claim, but it's also a criminal offense that can lead to severe penalties.
- Forgetting to include the OSHA Log Case Number, if applicable. This oversight can hinder the coordination between workplace safety records and compensation claims.
- Omitting or incorrectly filling out the Employee’s Occupation Description and Nature of Business. This information helps in understanding the context of the injury or illness.
- Incorrectly specifying the date and time of the injury, or the time the employee began work on the injury date. Accurate timing is essential for verifying claims and determining eligibility.
- Not detailing the how, what, when, and where of the incident in the description of how the injury or illness occurred. A detailed account supports a thorough assessment of the claim.
- Overlooking to specify if full wages were paid for the date of injury and failing to accurately report the employee's employment status (e.g., full-time, part-time, seasonal). This information is critical for calculating benefits.
- Neglecting to indicate if the injury or illness occurred on the employer’s premises. The location of the incident can influence the determination of the claim.
Avoiding these mistakes can help ensure that the claim process is smooth and that employees receive the support and compensation they're entitled to in a timely manner. Always double-check the form before submission and consult with a professional if uncertainties arise.
Documents used along the form
When handling workplace injuries in Tennessee, it's crucial to be thorough and precise in the documentation process. The "Tennessee First Report form" serves as a foundational document, but to ensure a comprehensive approach, several other forms and documents are often used in conjunction. Below is a brief description of each, illustrating their significance in the workflow of reporting and managing workplace injuries.
- Wage Statement Form: This document provides a detailed record of the injured employee's earnings over a specified period before the injury occurred. It's essential for calculating workers' compensation benefits.
- Employer’s Wage Verification Form: Similar to the Wage Statement Form, this document verifies the wages of the injured employee, but it is completed directly by the employer for accuracy in benefits calculation.
- Medical Authorization Release Form: This form grants permission for the release of the injured employee's medical records to the employer or insurance carrier, ensuring privacy laws are respected.
- Accident Investigation Report: This internal document allows employers to detail the circumstances of the injury, identifying potential safety risks and preventing future accidents.
- Panel of Physicians Form: It lists healthcare providers that an injured employee may choose from for their treatment, in compliance with Tennessee workers' compensation laws.
- Notice of Denial of Workers’ Compensation Benefits: This document is used if an employer or insurer decides to deny a worker's compensation claim, outlining the reasons for denial.
- Request for Assistance Form: Used by employees to seek help from the Tennessee Bureau of Workers’ Compensation if they encounter issues with their claim or need additional guidance.
Incorporating these documents alongside the Tennessee First Report form allows for a streamlined, transparent, and efficient process, ensuring both employee welfare and compliance with state regulations. It's a collaborative effort that underscores the importance of accurate documentation and communication between all parties involved in workplace injury management.
Similar forms
The Tennessee First Report form is closely related to the OSHA Injury and Illness Incident Report Form 301. Both documents serve as initial reports for workplace injuries or illnesses, collecting comprehensive information about the incident, including details about the employee involved, the nature of their injury or illness, and how the incident occurred. While the Tennessee form is specific to the state’s Department of Labor requirement under workers' compensation laws, Form 301 is used nationally for OSHA compliance, demonstrating the uniform need across different jurisdictions to document workplace incidents accurately and thoroughly.
Similarly, the First Report of Injury (FROI) form used across various states for workers’ compensation claims shares numerous similarities with Tennessee’s First Report form. Like Tennessee’s form, the FROI captures essential data about workplace injuries or illnesses, including the injured employee’s details, the injury or illness specifics, and employer information. Both forms initiate the workers’ compensation process by documenting the occurrence and serving as a formal notice to insurance carriers, although specific information requirements can vary slightly from state to state.
The DWC-1 Claim Form in California acts as another counterpart, facilitating workers' compensation claims within that state. This form also collects detailed information regarding the injured employee, the date, time, and nature of the injury or illness, along with the employer's details. Both the DWC-1 and the Tennessee First Report serve the same purpose of kickstarting the claims process by providing a structured way to report workplace incidents to insurers and state agencies, albeit tailored to meet the legal requirements of their respective states.
The Workers' Compensation First Notice of Injury form in Florida is another document that bears a resemblance to the Tennessee First Report form. It is designed to capture initial information about a workplace injury or illness to file a claim. Both documents are integral to their state’s workers' compensation system, requiring details on the employee, the incident, and subsequent medical treatment. This parallel structure underscores their shared goal of ensuring that injured workers receive appropriate medical care and compensation benefits promptly.
The Accident Report Form used by employers to report vehicle accidents involving their employees is conceptually similar to the Tennessee First Report form, albeit focused on a specific type of incident. Both forms gather detailed incident descriptions, including information about the individuals involved and the extent of injuries or damage. The main difference lies in the Accident Report Form's emphasis on vehicle details and circumstances of the accident, illustrating the adaptability of incident reporting to various contexts.
The Workers' Compensation Notice of Employee Injury Form in New York represents another example of a document with analogous objectives and content to Tennessee's First Report. It provides a framework for reporting employee injuries to commence the workers’ compensation process. While tailored to New York State’s requirements, it similarly requires detailed incident, employer, and employee information, showcasing a universal approach to injury reporting within workers’ compensation systems.
Employer's Report of Industrial Injury used in Arizona is akin to the Tennessee First Report of Work Injury or Illness in its function and content. This form is necessary for reporting workplace injuries in Arizona, detailing the incident, employee information, and the employer's account of the event. Both forms play a crucial role in their respective states’ efforts to manage and support workers' compensation claims, highlighting the importance of initial incident reporting in facilitating the claims process.
The Incident Report Forms that schools use to document injuries or incidents involving students or staff mirror the Tennessee First Report form in structure and purpose. While targeted towards educational institutions rather than workplaces, these forms also aim to capture a comprehensive record of what happened, who was involved, and the outcome. This similarity underscores the universal need across different environments to have a structured method for reporting and documenting incidents to ensure appropriate responses and interventions.
Dos and Don'ts
When completing the Tennessee First Report form for a work injury or illness, it is crucial to adhere to guidelines that ensure accuracy, compliance, and integrity throughout the process. Here are key dos and don'ts to consider:
Do:- Provide complete information: Ensure every field is filled out accurately. Incomplete forms may result in delays or complications in the processing of the claim.
- Report in a timely manner: Submit the form immediately after the incident to your insurance carrier to avoid any unnecessary delays in the claim process.
- Double-check for accuracy: Before submission, verify all details, especially numbers and dates, to ensure they are correct.
- Describe the incident clearly: Include a detailed description of how the injury or illness occurred, the body part affected, and the direct cause, providing clarity and avoiding ambiguity.
- Adhere to legal guidelines: Understand that it's a legal requirement to fill out this form truthfully and accurately to avoid penalties, including imprisonment, fines, and denial of benefits.
- Seek clarification if needed: Utilize resources such as the Benefit Review System or contact a Workers' Compensation Specialist if you have any questions or require assistance with the form.
- Provide false information: Knowingly submitting false, incomplete, or misleading information is considered fraud and is subject to severe penalties.
- Omit the preparer’s information: Make sure to include the name, title, company name, and phone number of the person preparing the report to ensure accountability.
- Ignore body part and nature of the injury codes: Use the correct codes for the body part affected and the nature of the injury to ensure clarity and facilitate processing.
- Forget to specify treatment details: Clearly indicate whether initial treatment was administered, and if so, the type of treatment received, including if hospitalization was required.
- Delay notification to your insurance carrier: Delaying this step could complicate the claim process for all parties involved.
- Be vague in describing the incident: Avoid ambiguity in explaining the circumstances surrounding the injury or illness as it may lead to misunderstandings or delays in the claim process.
Misconceptions
When dealing with the Tennessee First Report form for work-related injuries or illnesses, employers and employees often encounter misconceptions. Understanding these misconceptions is crucial for accurate reporting and ensuring that all parties are informed about their responsibilities and rights under Tennessee Workers' Compensation Law. Here are eight common misunderstandings:
- Only serious injuries need to be reported: All work-related injuries or illnesses, regardless of their severity, must be reported. This ensures that even minor injuries are documented, which can become significant if complications arise.
- It's only necessary to report if the employee misses work: Even if the employee does not miss any work, the injury or illness must be reported. This includes incidents where no immediate medical treatment is required.
- The form is optional: Contrary to what some may believe, using this form is mandatory under Tennessee Workers' Compensation Law for reporting work-related injuries or illnesses.
- Employers are responsible for deciding if an injury is work-related: While employers play a critical role in the reporting process, it's up to medical professionals and, ultimately, the insurance carrier or the Tennessee Department of Labor to determine if an injury or illness is work-related.
- Reporting an injury will always lead to higher insurance premiums: Insurance premiums are influenced by numerous factors, and a single report may not necessarily increase rates. It's important to focus on maintaining a safe work environment to prevent injuries.
- Employees can be retaliated against for reporting: Tennessee law protects employees from retaliation for reporting work-related injuries or illnesses. Employers must not discourage employees from reporting.
- The form must be completed by the employee: It is the employer's responsibility to complete and file the form with their insurance carrier, not the injured or ill employee's.
- Fraud concerns limit what should be reported: It's essential to report all factual information related to the work-related injury or illness. Falsifying or omitting information to avoid potential fraud accusations does more harm than good, and penalties for fraud are serious.
By dispelling these misconceptions, employers and employees can navigate the complexities of work-related injury and illness reporting with greater confidence and clarity.
Key takeaways
When dealing with a workplace injury or illness in Tennessee, proper documentation is crucial for compliance with state regulations and to ensure the well-being of the employee. The Tennessee Department of Labor and Workforce Development requires employers to complete the Employer’s First Report of Work Injury or Illness form. Here are some key takeaways about filling out and using this form:
- Timeliness is key: The form should be filed with your insurance carrier immediately after the notification of an injury. This prompt action helps to ensure that claims are processed efficiently, supporting a quicker resolution for the injured employee.
- Accuracy matters: It's important to provide accurate and complete information. The form warns that providing false, incomplete, or misleading information is a criminal offense that can result in penalties, including imprisonment, fines, and denial of insurance benefits.
- Details of the incident: The form requires a thorough description of how the injury or illness occurred. This includes detailing the employee’s activity just before the incident, the part of the body affected, and how it was affected, as well as any object or substance that directly caused harm to the employee.
- Seek guidance if needed: For questions or assistance, the state offers a Benefit Review System. Employers or their representatives can call a specified toll-free number to speak with a worker's compensation specialist. This resource can be invaluable in navigating the workers' compensation process and ensuring compliance with state requirements.
Completing the Tennessee First Report form accurately and promptly can significantly influence the outcome of a workers' compensation claim. It not only aids in the administrative process but also plays a critical role in ensuring that employees receive the appropriate care and benefits in the event of a workplace injury or illness.
Popular PDF Documents
Massachusetts Tax Payment - Ensures that Massachusetts state transactions are conducted in accordance with all relevant laws and regulations, safeguarding public funds.
Moneygram Refund Form - Provide your complete name, contact, and address information to pay a bill or load a prepaid card with ease.