Get Healthfirst Eft Era Authorization Form
The Healthfirst EFT/ERA Authorization Form is a crucial document for healthcare providers who wish to manage their financial transactions with Healthfirst more efficiently. Updated on November 17, 2006, this form allows providers to choose between different types of transactions, such as adding or changing Electronic Funds Transfers (EFTs) and Electronic Remittance Advices (ERAs), or terminating them altogether. Providers are required to fill out this form once per Tax ID, with the condition that all providers under the group share the same bank account. Additionally, a list of provider IDs at the payee entity level must be attached for the authorization to be applied correctly. The form facilitates the crediting of transactions to the provider's bank account, requiring details such as account type, bank name, and account number, alongside a necessity for a deposit slip or cancelled check if participating in EFT. It further outlines the selection process for those looking to partake in the ERA process, mentioning the need for a clearinghouse and the options available. A unique aspect of this form is the provider's authorization for Healthfirst to initiate credit entries and adjustments, which remains effective until a written termination notice is provided, giving Healthfirst and the depositing bank reasonable time to act on the termination. Providers have the option to receive only ERA after a grace period, emphasizing the shift towards electronic transactions. The form concludes with sections for provider and contact person information, ensuring a straightforward communication channel for any queries or updates related to the EFT/ERA Authorization process. This streamlined approach not only intends to ease the financial operations for providers but also aligns with Healthfirst's policies, highlighting an ongoing effort to enhance service delivery and operational efficiency.
Healthfirst Eft Era Authorization Example
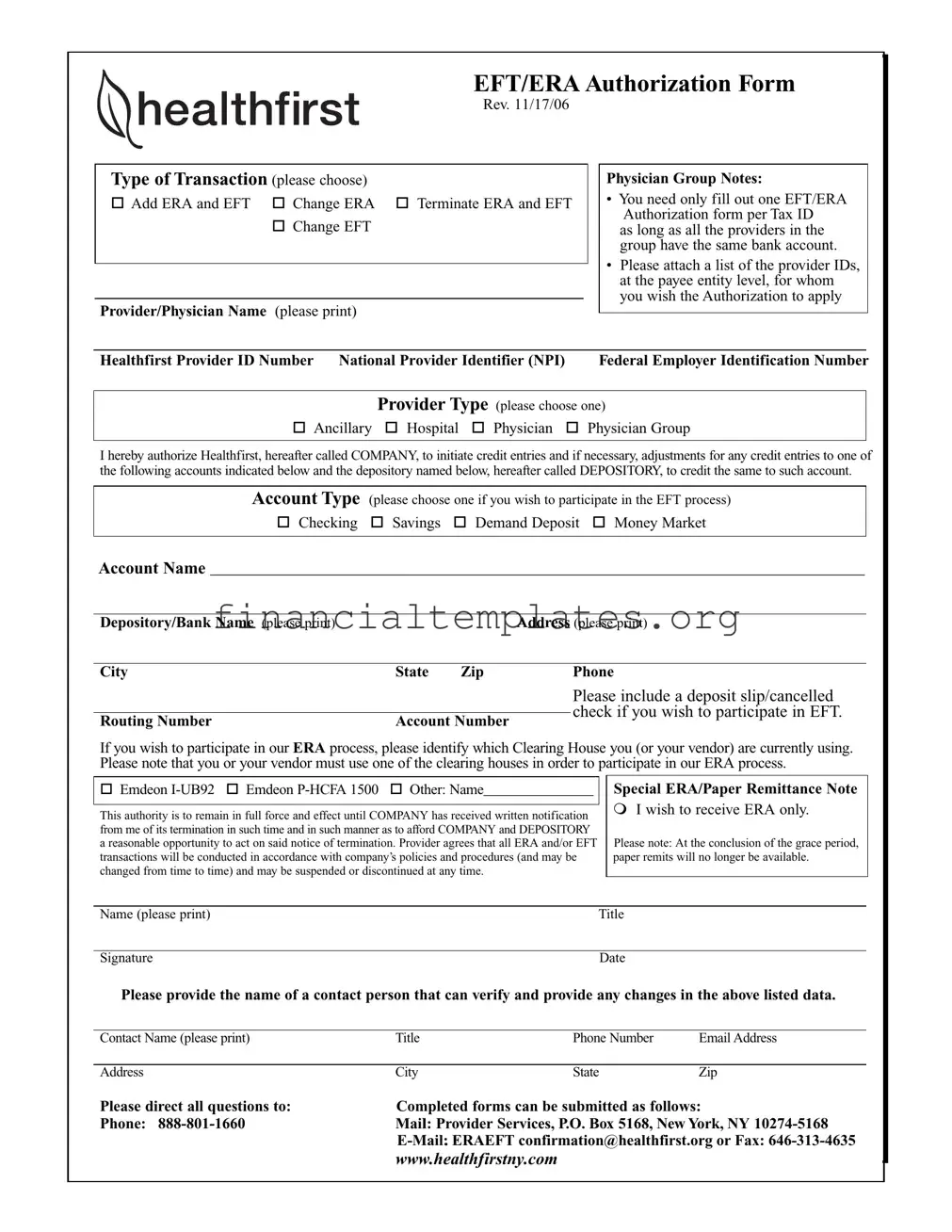
EFT/ERA Authorization Form
Rev. 11/17/06
Type of Transaction (please choose)
Add ERA and EFT |
Change ERA |
Terminate ERA and EFT |
|
Change EFT |
|
Provider/Physician Name (please print)
Physician Group Notes:
•You need only fill out one EFT/ERA Authorization form per Tax ID
as long as all the providers in the group have the same bank account.
•Please attach a list of the provider IDs, at the payee entity level, for whom you wish the Authorization to apply
Healthfirst Provider ID Number NATIONAL PROVIDER IDENTIFIER (NPI) |
Federal Employer Identification Number |
|||
|
|
|||
|
Provider Type (please choose one) |
|
||
Ancillary |
Hospital |
Physician |
Physician Group |
|
|
|
|
|
|
I hereby authorize Healthfirst, hereafter called COMPANY, to initiate credit entries and if necessary, adjustments for any credit entries to one of the following accounts indicated below and the depository named below, hereafter called DEPOSITORY, to credit the same to such account.
Account Type (please choose one if you wish to participate in the EFT process)
Checking Savings Demand Deposit Money Market
Account Name _____________________________________________________________________________________
Depository/Bank Name (please print) |
|
|
Address (please print) |
|
|
|
|
|
|
City |
State |
Zip |
|
Phone |
|
|
|
|
Please include a deposit slip/cancelled |
|
|
|
|
check if you wish to participate in EFT. |
Routing Number |
Account Number |
|
||
|
|
|||
If you wish to participate in our ERA process, please identify which Clearing House you (or your vendor) are currently using. Please note that you or your vendor must use one of the clearing houses in order to participate in our ERA process.
Emdeon |
Emdeon |
Other: Name_______________ |
This authority is to remain in full force and effect until COMPANY has received written notification from me of its termination in such time and in such manner as to afford COMPANY and DEPOSITORY a reasonable opportunity to act on said notice of termination. Provider agrees that all ERA and/or EFT transactions will be conducted in accordance with company’s policies and procedures (and may be changed from time to time) and may be suspended or discontinued at any time.
Special ERA/Paper Remittance Note
I wish to receive ERA only.
Please note: At the conclusion of the grace period, paper remits will no longer be available.
Name (please print) |
Title |
|
|
Signature |
Date |
Please provide the name of a contact person that can verify and provide any changes in the above listed data.
Contact Name (please print) |
Title |
Phone Number |
Email Address |
|
|
|
|
Address |
City |
State |
Zip |
Please direct all questions to: |
Completed forms can be submitted as follows: |
||
Phone: |
Mail: Provider Services, P.O. Box 5168, New York, NY |
||
|
|||
www.healthfirstny.com
Document Specifics
| Fact Number | Detail |
|---|---|
| 1 | The Healthfirst EFT/ERA Authorization Form was last revised on November 17, 2006. |
| 2 | Providers can choose among different types of transactions such as Add ERA and EFT, Change ERA, Terminate ERA and EFT, or Change EFT. |
| 3 | Only one EFT/ERA Authorization form is needed per Tax ID if all providers in the group share the same bank account. |
| 4 | A list of provider IDs at the payee entity level must be attached for the Authorization to apply. |
| 5 | Providers must select a provider type from the options provided: Ancillary, Hospital, Physician, or Physician Group. |
| 6 | To participate in the EFT process, providers can choose between account types: Checking, Savings, Demand Deposit, and Money Market. |
| 7 | For ERA participation, providers or their vendors must use an approved clearing house. |
| 8 | The authorization remains effective until Healthfirst receives written notification of its termination. |
| 9 | ERA and/or EFT transactions are subject to Healthfirst's policies and procedures and can be revised, suspended, or discontinued at any time. |
| 10 | The form provides contact information for inquiries and specifies where completed forms can be submitted: by phone, mail, e-mail, or fax. |
Guide to Writing Healthfirst Eft Era Authorization
Getting started with the Healthfirst EFT/ERA Authorization form is a straightforward process aimed at enabling providers to efficiently manage payments and remittance advice electronically. By accurately completing and submitting this form, providers can facilitate the automatic deposit of payments into the designated bank account and receive electronic remittance advice, simplifying the reconciliation process. Below are the steps to correctly fill out and submit the Healthfirst EFT/ERA Authorization form.
- Choose the Type of Transaction by selecting either "Add ERA and EFT", "Change ERA", "Terminate ERA and EFT", or "Change EFT".
- Print the Provider/Physician Name clearly in the provided space.
- Under Notes, attach a list of provider IDs at the payee entity level if the authorization applies to multiple providers within the same group sharing the same Tax ID and bank account.
- Fill in the Healthfirst Provider ID Number, NATIONAL PROVIDER IDENTIFIER (NPI), and Federal Employer Identification Number.
- Select the Provider Type that applies: Ancillary, Hospital, Physician, or Physician Group.
- Authorize Healthfirst to initiate credit entries by choosing the Account Type you wish to use for EFT (Checking, Savings, Demand Deposit, Money Market).
- Provide the Account Name, Depository/Bank Name, its full address (city, state, zip), and phone number. Attach a deposit slip or canceled check to participate in EFT.
- Enter the Routing Number and Account Number for the account where funds should be deposited.
- To participate in the ERA process, indicate which Clearing House you or your vendor use. Options include Emdeon I-UB92, Emdeon P-HCFA 1500, or specify another if applicable.
- If you wish to receive ERA only, make sure to select the special ERA/Paper Remittance Note option.
- Print the Name and Title of the signatory, provide a Signature and the Date.
- Fill in the contact information of a person who can verify and provide any changes to the data provided in the form, including Contact Name (printed), Title, Phone Number, and Email Address, along with their Address, City, State, and Zip.
- Review all information for accuracy and completeness before submitting the form via Phone, Mail, Email, or Fax to the contact details provided on the form.
After the form is submitted, it is essential to wait for confirmation from Healthfirst. The successful processing of the EFT/ERA Authorization form will streamline your electronic transactions with Healthfirst, making your financial operations more efficient and less time-consuming.
Understanding Healthfirst Eft Era Authorization
How do I choose the right type of transaction on the Healthfirst EFT/ERA Authorization Form?
To select the correct transaction type, please understand the options: Add ERA and EFT if you are starting new electronic funds transactions and electronic remittance advices with Healthfirst; Change ERA if you need to update information or bank details for your electronic remittance advices; Terminate ERA and EFT if you wish to stop these electronic services; and Change EFT if your bank information for electronic funds transfers needs to be updated. Choose based on your current needs.
Can one EFT/ERA Authorization Form cover all providers in a group?
Yes, a single form can cover all providers in a group if they share the same Tax ID and bank account. It is required to attach a list of the provider IDs at the payee entity level that the authorization will apply to. This makes the process efficient for groups managing their banking and payment processes centrally.
What should I include with the form to participate in the EFT process?
To participate in the EFT process, you must include a deposit slip or a cancelled check with the form. This is necessary to verify your bank account details, such as the account name, depository/bank name, routing number, and account number, ensuring accurate and secure transactions.
How do I enroll in the Electronic Remittance Advice (ERA) process?
To enroll in the ERA process, identify which Clearing House you or your vendor currently use. Healthfirst requires participation through one of their recognized clearing houses to process ERAs. If your clearing house is not listed, please select “Other” and provide its name. This step is crucial for setting up electronic remittance advices correctly.
What happens at the end of the grace period if I choose ERA only?
If you choose to receive ERA only, be aware that paper remittances will no longer be available after the grace period concludes. This means you will exclusively receive remittance advices in an electronic format, aligning with efforts to streamline the payment and reconciliation process. If you rely on paper remittances, ensure you are prepared for this transition.
Common mistakes
When completing the Healthfirst EFT/ERA Authorization form, individuals often make several mistakes that can lead to delays or errors in processing. Avoid these common errors to ensure the form is processed smoothly:
Not selecting the Type of Transaction at the beginning of the form. It's crucial to indicate whether you're adding, changing, or terminating ERA and EFT to guide the processing accurately.
Failing to attach a list of provider IDs for whom the Authorization applies, especially if the form is being submitted for a physician group under one Tax ID. This list is essential for Healthfirst to apply the authorization correctly.
Omitting the inclusion of a deposit slip or cancelled check when opting to participate in the EFT process. This documentation is required to verify the account information provided on the form.
Not specifying a Clearing House if choosing to participate in the ERA process. This information is necessary for Healthfirst to route ERA transactions through the appropriate channels.
Inadequate notification regarding termination. The form must be submitted in such a manner and time frame that allows the company and the depository bank a reasonable opportunity to act on the termination notice.
By paying close attention to these details, individuals can streamline the submission process, helping ensure that the electronic funds transfers and electronic remittance advice transactions are handled efficiently and accurately.
Documents used along the form
When healthcare providers choose to enroll in Electronic Funds Transfer (EFT) and Electronic Remittance Advice (ERA) with Healthfirst, it simplifies the financial and administrative operations significantly. This not only modernizes the process of payment and record-keeping but also ensures a seamless transaction flow, making financial management more efficient. Alongside the Healthfirst EFT/ERA Authorization form, several other forms and documents are crucial for a complete and operative setup of these transactions.
- W-9 Form: This form is crucial as it provides the Taxpayer Identification Number (TIN) and certification, ensuring that the correct entity receives payments and adheres to tax reporting requirements. This information must match the details provided on the EFT/ERA Authorization form to avoid any discrepancies in payment processing.
- Direct Deposit Authorization Form: While the EFT/ERA Authorization form initiates the process, a Direct Deposit Authorization form is often required by the banking institution. This form provides explicit authorization to deposit funds directly into the bank account specified by the healthcare provider or practice.
- Clearinghouse Enrollment Forms: Since the ERA component requires the use of a clearinghouse, providers need to fill out enrollment forms for their chosen clearinghouse if they have not previously established a relationship. This facilitates the electronic exchange of healthcare information, including remittance advice documents.
- Bank Verification Letter: A bank verification letter may be requested to confirm the account details provided for EFT. This letter, typically issued by the bank, verifies the account name, number, and the routing number, ensuring that the details match those on the EFT/ERA Authorization form and reducing the risk of payment redirection.
It's essential for healthcare providers to accurately complete and submit these documents in conjunction with the Healthfirst EFT/ERA Authorization form. Each document serves an integral role in establishing and maintaining the flow of electronic funds and information between healthcare providers, their financial institutions, and Healthfirst. By doing so, the providers ensure that the setup process is as smooth as possible, leading to a timely and efficient system for receiving payments and remittance advice, ultimately enhancing the overall efficiency of healthcare administration.
Similar forms
The Automatic Clearing House (ACH) Authorization Form is very similar to the Healthfirst EFT/ERA Authorization Form. Both forms authorize financial transactions between businesses and financial institutions. The ACH Authorization Form, like the Healthfirst form, is used to grant permission for automatic deposits or withdrawals, requiring the account holder's information, financial institution details, and a signed agreement to initiate transactions.
A Direct Deposit Authorization Form shares similarities as well, chiefly in allowing employers to deposit funds directly into an employee's bank account. Similar to the EFT section of the Healthfirst form, this document requires the recipient's bank account details, including the routing and account numbers, to set up the payment process. Both forms ensure that funds are transferred electronically, streamlining financial transactions for both parties involved.
The Electronic Funds Transfer (EFT) Agreement is another document closely related to the Healthfirst EFT/ERA Authorization Form. This agreement outlines the terms and conditions under which electronic transactions will occur between two parties. Like the Healthfirst form, it necessitates bank account information, authorization by the account holder, and specifies the process for making adjustments or terminating the agreement.
The Vendor Direct Deposit Authorization Form also parallels the Healthfirst form, facilitating vendor payments via direct deposit. This form collects vendor banking information to automate payments, similar to how health care providers submit their information to Healthfirst for EFT. Both documents streamline financial operations, reducing the reliance on physical checks.
The ERA Enrollment Form is specific to the health care industry, like parts of the Healthfirst document, and allows providers to receive Electronic Remittance Advice instead of paper statements. These forms collect provider information and specify preferences for receiving payment information electronically, promoting efficiency and environmental sustainability by reducing paper use.
A Health Insurance Portability and Accountability Act (HIPAA) Authorization Form, while primarily focused on the privacy and security of patient information, shares an emphasis on regulatory compliance with the Healthfirst form. In the context of EFT/ERA transactions, both documents adhere to standards that protect sensitive financial and personal information during electronic transactions.
The Payment Card Authorization Form is akin to the EFT authorization section of the Healthfirst form, but for credit card transactions. It allows businesses to charge a customer's credit card for services rendered, requiring the cardholder's permission and billing information. Although used in different contexts, both forms permit the electronic transfer of funds from an individual or entity to another.
Finally, the Medical Claims Processing Authorization Form, which permits an insurer or third-party administrator to process health care claims on behalf of a provider or patient, is conceptually related to the Healthfirst form's ERA process. It involves the electronic handling of claim information and payments, necessitating provider information and consent to engage in electronic transactions, promoting efficiency in the health care billing cycle.
Dos and Don'ts
When completing the Healthfirst EFT/ERA Authorization form, it's important to follow a set of guidelines to ensure accurate and efficient processing. Below are the things you should and shouldn't do:
DO:
- Double-check that all information is accurate, especially bank details like the routing and account numbers, to avoid any delays or issues with transactions.
- Ensure that the provider name and Tax ID are correctly entered to maintain consistency across all documents.
- Include a list of provider IDs if the authorization applies to multiple providers under the same Tax ID to streamline the process.
- Attach a voided check or deposit slip if you wish to participate in EFT, as this can help confirm your bank account details.
- Clearly mark your selection for the type of transaction you're requesting (Add, Change, Terminate) for both ERA and EFT to avoid confusion.
- Sign and date the form to validate the authorization. Without a signature, the form may not be processed.
- Provide a contact person's details for any follow-up or clarification needed.
DON'T:
- Leave any required fields blank. Incomplete forms can lead to processing delays or even rejections.
- Assume all sections apply to you. If a section is not relevant to your request, make sure to skip or indicate it's not applicable.
- Use outdated information for the contact person, banking details, or provider information as this could lead to incorrect processing.
- Forget to specify your clearinghouse if participating in the ERA process, as this is vital for proper electronic remittance advice transactions.
- Ignore the need to notify the company in writing for termination of the authorization, as verbal notices are not accepted.
- Submit the form without checking if there have been any updates or changes to the process that might affect your submission.
- Misplace the contact information for questions (Provider Services), as you might need it for inquiries or assistance.
Misconceptions
There are several misconceptions about the Healthfirst EFT/ERA Authorization form that healthcare providers and their administrative staff should be aware of. Clearing up these misunderstandings can streamline the process and ensure timely and accurate transactions.
- Misconception 1: Different forms are needed for each provider within a group.
Contrary to this belief, only one EFT/ERA Authorization form is required per Tax ID, assuming all providers in the group utilize the same bank account. This simplifies the process and reduces paperwork. - Misconception 2: Attachments such as deposit slips or canceled checks are optional for EFT participation.
In fact, including a deposit slip or canceled check is crucial for those wishing to partake in the EFT process. This documentation is necessary for verifying account information to ensure accurate and efficient transactions. - Misconception 3: The ERA process does not require the use of a clearing house.
This is incorrect. Participation in the ERA process mandates the use of one of the listed clearing houses. It is essential for providers or their vendors to work with a recognized clearing house to facilitate ERA transactions. - Misconception 4: Written notification of termination is not strictly required.
On the contrary, Healthfirst must receive written notification of any termination to afford the company and the depository adequate time to act upon it. This formal communication is necessary to end the authorization officially and avoid any unwanted transactions.
Understanding and addressing these misconceptions can help ensure that healthcare providers efficiently and effectively manage their EFT/ERA authorization with Healthfirst, minimizing financial disruptions and maintaining operational smoothness.
Key takeaways
Understanding the Healthfirst EFT/ERA Authorization form is essential for providers and their billing operations. Here are key takeaways to ensure the process is completed correctly and efficiently:
- Single Form Sufficiency: Only one EFT/ERA Authorization form is required per Tax ID, provided all providers within the group share the same bank account.
- Provider ID List Attachment: Alongside the form, attach a list of all the provider IDs (at the payee entity level) that the authorization will cover.
- Bank Account Information: Clearly indicate your chosen bank account type and provide the account name, bank name, address, routing number, and account number. Ensure the bank account details are accurate to enable smooth credit entries and adjustments.
- Deposit Slip/Cancelled Check Requirement: Submitting a deposit slip or a cancelled check is necessary if you wish to participate in the EFT process, serving as verification of your account details.
- Clearing House Details for ERA: If you opt into the ERA process, specify the clearing house you or your vendor are using. This information is critical to facilitate ERA transactions.
- Authorization Termination: The form stays in effect until Healthfirst receives written notification of its termination, allowing reasonable time for the company and depository to act upon it.
- Contact Information: Provide the name, title, phone number, and email address of a contact person who can verify and provide updates to the information submitted.
Following these guidelines will help ensure that your EFT/ERA transactions with Healthfirst are set up correctly, facilitating timely and accurate payments.
Popular PDF Documents
Sample Loan Application - The inclusion of a signature field reinforces the seriousness and formal nature of the mortgage application process.
IRS 8889 - It includes a section for reporting employer contributions to an individual’s HSA.