Get First Report Of Injury Or Illness Form
The First Report of Injury or Illness form is a critical document in the sphere of workers' compensation, providing a systematic way to record incidents of work-related injuries or illnesses. This form, crucial for both employers and employees, acts as the initial notification that sets the workers' compensation claim process in motion. It captures essential details, including jurisdiction specific information, employer and employee identification, the nature and circumstances of the incident, initial medical treatment data, and any subsequent actions taken following the injury or illness. The comprehensive nature of this form ensures that a detailed account of the occurrence is documented, which is valuable for all involved parties. It not only aids in the administration of the workers' compensation claim but also plays a role in compliance with state regulations concerning workplace injuries and illnesses. Employers are obligated to maintain such records as part of their broader responsibilities under various occupational safety and health acts, contributing to a safer work environment by identifying potential hazards and preventing future incidents.
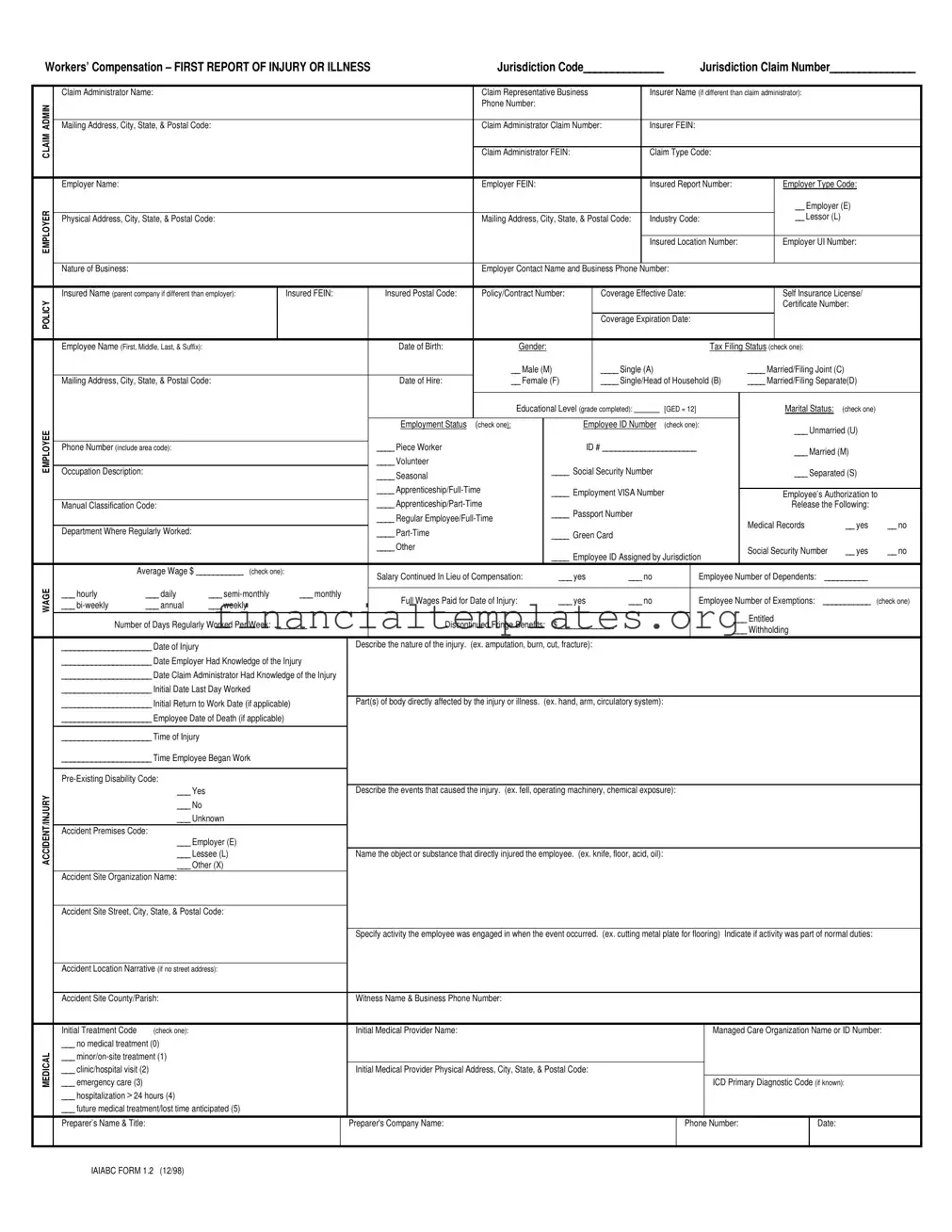
First Report Of Injury Or Illness Example
Workers’ Compensation – FIRST REPORT OF INJURY OR ILLNESS |
Jurisdiction Code______________ |
|
|
Jurisdiction Claim Number_______________ |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Claim Administrator Name: |
|
|
|
|
|
|
Claim Representative Business |
|
Insurer Name (if different than claim administrator): |
|
|
|
|||||||||||
ADMIN |
|
|
|
|
|
|
|
|
Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Mailing Address, City, State, & Postal Code: |
|
|
|
|
|
Claim Administrator Claim Number: |
Insurer FEIN: |
|
|
|
|
|
|
|||||||||||
CLAIM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Claim Administrator FEIN: |
|
Claim Type Code: |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Employer Name: |
|
|
|
|
|
|
|
Employer FEIN: |
|
|
|
Insured Report Number: |
|
Employer Type Code: |
|
||||||||
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__ Employer (E) |
|
|||
|
Physical Address, City, State, & Postal Code: |
|
|
|
|
|
Mailing Address, City, State, & Postal Code: |
Industry Code: |
|
__ Lessor (L) |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insured Location Number: |
|
Employer UI Number: |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Nature of Business: |
|
|
|
|
|
|
|
Employer Contact Name and Business Phone Number: |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Insured Name (parent company if different than employer): |
|
Insured FEIN: |
|
Insured Postal Code: |
Policy/Contract Number: |
Coverage Effective Date: |
|
Self Insurance License/ |
|
||||||||||||||
POLICY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Certificate Number: |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Coverage Expiration Date: |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee Name (First, Middle, Last, & Suffix): |
|
|
|
|
|
Date of Birth: |
Gender: |
|
|
|
|
|
|
|
Tax Filing Status (check one): |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
__ Male (M) |
____ Single (A) |
|
|
|
|
____ Married/Filing Joint (C) |
|
||||||||
|
Mailing Address, City, State, & Postal Code: |
|
|
|
|
Date of Hire: |
__ Female (F) |
____ Single/Head of Household (B) |
____ Married/Filing Separate(D) |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Educational Level (grade completed): _______ |
[GED = 12] |
|
Marital Status: |
(check one) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
EMPLOYEE |
|
|
|
|
|
|
|
Employment Status |
(check one): |
|
|
Employee ID Number |
(check one): |
|
___ Unmarried (U) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone Number (include area code): |
|
|
|
|
|
____ Piece Worker |
|
|
|
ID # ______________________ |
|
___ Married (M) |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
____ Volunteer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupation Description: |
|
|
|
|
|
|
____ Seasonal |
|
|
____ Social Security Number |
|
|
|
|
|
___ Separated (S) |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____ |
|
____ Employment VISA Number |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee’s Authorization to |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Manual Classification Code: |
|
|
|
|
|
____ |
|
____ Passport Number |
|
|
|
|
|
|
Release the Following: |
|
|||||||
|
|
|
|
|
|
|
|
____ Regular |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical Records |
|
__ yes |
__ no |
||||
|
Department Where Regularly Worked: |
|
|
|
|
|
____ |
|
|
____ Green Card |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
____ Other |
|
|
|
|
|
|
|
|
|
|
Social Security Number |
__ yes |
__ no |
|||
|
|
|
|
|
|
|
|
|
|
|
____ Employee ID Assigned by Jurisdiction |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Average Wage $ ___________ (check one): |
|
Salary Continued In Lieu of Compensation: |
|
___ yes |
___ no |
|
|
Employee Number of Dependents: |
__________ |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
WAGE |
___ hourly |
___ daily |
___ |
|
___ monthly |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Full Wages Paid for Date of Injury: |
|
___ yes |
___ no |
|
|
Employee Number of Exemptions: |
___________ |
(check one) |
||||||||||||||
|
___ |
___ annual |
___ weekly |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Entitled |
|
|
|
|||
|
Number of Days Regularly Worked Per Week: |
_______ |
|
|
Discontinued Fringe Benefits: |
$_____________ |
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
___ Withholding |
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
_____________________ Date of Injury |
|
|
|
|
Describe the nature of the injury. (ex. amputation, burn, cut, fracture): |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
_____________________ Date Employer Had Knowledge of the Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
_____________________ Date Claim Administrator Had Knowledge of the Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
_____________________ Initial Date Last Day Worked |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
_____________________ Initial Return to Work Date (if applicable) |
Part(s) of body directly affected by the injury or illness. (ex. hand, arm, circulatory system): |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
_____________________ Employee Date of Death (if applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____________________ Time of Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____________________ Time Employee Began Work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
ACCIDENT/INJURY |
|
___ Yes |
|
|
|
|
Describe the events that caused the injury. (ex. fell, operating machinery, chemical exposure): |
|
|
|
|
|
|
|||||||||||
|
___ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Premises Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Employer (E) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Lessee (L) |
|
|
|
Name the object or substance that directly injured the employee. (ex. knife, floor, acid, oil): |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
___ Other (X) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Site Organization Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Accident Site Street, City, State, & Postal Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
Specify activity the employee was engaged in when the event occurred. (ex. cutting metal plate for flooring) Indicate if activity was part of normal duties: |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Accident Location Narrative (if no street address): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Accident Site County/Parish: |
|
|
|
|
Witness Name & Business Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Initial Treatment Code |
(check one): |
|
|
|
|
Initial Medical Provider Name: |
|
|
|
|
|
|
|
|
|
Managed Care Organization Name or ID Number: |
|||||||
|
___ no medical treatment (0) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL |
___ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ emergency care (3) |
|
|
|
|
|
Initial Medical Provider Physical Address, City, State, & Postal Code: |
|
|
|
|
|
ICD Primary Diagnostic Code (if known): |
|
|||||||||||
|
___ clinic/hospital visit (2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
___ hospitalization > 24 hours (4) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ future medical treatment/lost time anticipated (5) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Preparer’s Name & Title: |
|
|
|
|
|
Preparer's Company Name: |
|
|
|
|
|
|
|
Phone Number: |
|
|
|
Date: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IAIABC FORM 1.2 (12/98)
Mail to: DIVISION OF WORKERS' COMPENSATION |
STATE OF IOWA |
DIVISION OF LABOR SERVICES |
|
1000 E GRAND |
EMPLOYERS WORK INJURY REPORT |
1000 E GRAND |
|
DES MOINES, IOWA 50319 |
EMPLOYERS FIRST REPORT OF INJURY |
DES MOINES, IOWA 50319 |
|
|
|
||
This section is to provide information valuable in handling this claim.
The Iowa Occupational Safety and Health Act
The following is a summary of the recordkeeping, reporting and posting responsibilities of employers under Iowa’s Occupational Safety and Health Act.
RECORDKEEPING REQUIREMENTS
Regulations issued under the Iowa Occupational Safety and Health Act of 1972 require establishments subject to the Act to maintain records of recordable occupational injuries and illness. Such records must consist of: (a) a log and summary of occupational injuries and illnesses and (b) a supplementary record of each occupational injury and illness.
LOG AND SUMMARY OF OCCUPATIONAL INJURIES AND ILLNESSES. Each recordable occupational injury and occupational illness must be entered on a log and summary of cases (0SHA Form No. 200) as early as practicable but no later than 6 working days after receiving information that a recordable case has occurred. A
SUPPLEMENTARY RECORD OF OCCUPATIONAL INJURIES AND ILLNESSES. To supplement the Log and Summary of Occupational Injuries and Illnesses, each employer must have available a record for each occupational injury or illness at each establishment within 6 working days after receiving information that a recordable case has occurred, OSHA Form No. 101 may be used for this purpose. State of Iowa Form No
ANNUAL SUMMARY. Each employer subject to the recordkeeping requirements must prepare a summary of the occupational injury and illness experience of the employees in each of the employer’s establishments at the end of each year based on the information contained in the log and summary of occupational injuries and illnesses for the particular establishment. OSHA Form No. 200 shall be used for this purpose. The summary shall be signed and posted in a place accessible to the employees no later than February 1 and shall remain in place until March 1. For employees who do not report to work at a single establishment, or who do not report to any fixed establishment on a regular basis, employers shall satisfy the posting requirement by presenting or mailing a copy of the annual summary during the month of February to all such employees who receive pay during that month. Summaries must be retained for 5 years following the end of the calendar year to which they relate.
EMPLOYEES NOT IN FIXED ESTABLISHMENTS. Employers of employees engaged in physically dispersed operations such as occur in construction, installation, repair or service activities who do not report to any fixed establishment on a regular basis but are subject to common supervision may satisfy the recordkeeping provisions with respect to such employees by:
(a)Maintaining the required records for each operation or group of operations which is subject to common supervision (field superintendent, field supervision, etc.) in an established central place;
(b)Having the address and telephone number of the central place available at each worksite; and
(c)Having personnel available at the central place during normal business hours to provide information from the records maintained there by telephone and by mail.
(Note: This regulation does not automatically apply to all construction, installation, repair or service activities. If in doubt about applicability to your operations, contact the Iowa Division of Labor Services.)
Records for personnel who do not primarily report or work at a single establishment, and who are generally not supervised in their daily work, such as traveling salespersons, technicians, engineers, etc., shall be maintained at the location from which they are paid or the base from which personnel operate to carry out their activities.
REPORTING REQUIREMENTS
Regulations issued under the Iowa Occupational Safety and Health Act require all employers subject to the Act to report in writing to the Iowa Workers' Compensation Commissioner any occupational injury or illness which temporarily disables an employee for more than three days or which results in permanent total disability, permanent partial disability, or death. State of Iowa Form No.
Iowa Division of Workers' Compensation shall forward all such reports to the Iowa Division of Labor Services.
In addition, employers must report to the Iowa Labor Commissioner within 8 hours each accident or health hazard that results in one or more fatalities or hospitalization of three or more employees. The toll free number that is available 24 hours a day, including weekends and holidays, to use to report is
Those establishments selected to participate in the annual Occupational Injuries and Illnesses Survey will be required to prepare a report (OSHA Form No
POSTING REQUIREMENTS
The Iowa Occupational Safety and Health Act requires that employees be informed of the job safety and health protection provided under the Act. The poster, “Safety and Health Protection on the Job,” is to be used for this purpose, and must be posted in a prominent place in the establishment to which the employees usually report to work. The poster briefly states the intent and coverage of the Act and the responsibilities of employers and employees to maintain safe and healthful working conditions.
EMPLOYERS WHO MUST KEEP OSHA RECORDS
Employers with 11 or more employees (at any one time in the previous calendar year) in the following industries must keep OSHA records. The industries are identified by name and by the appropriate Standard Industrial Classification (SIC) code:
•Agriculture, forestry, and fishing (SIC’s
•Oil and gas extraction (SIC 13 and 1477)
•Construction (SIC’s
•Manufacturing (SIC’s
•Transportation and public utilities (SIC’s
•Wholesale trade (SIC’s
•Building materials and garden supplies (SIC 52)
•General merchandise and food stores (SIC’s 53 and 54)
•Hotels and other lodging places (SIC 70)
•Repair services (SIC’s 75 and 76)
•Amusement and recreation services (SIC 79)
•Health services (SIC 80), and
•State and local government (Above SIC ‘s plus
If employers in any of the industries listed above have more than one establishment with combined employment of 11 or more employees, records must be kept for each individual establishment.
All employers, including small employers and those in exempted SIC’s, must continue to meet the requirement to report fatalities or multiple (3 or more) hospitalizations and all occupational injuries or occupational illnesses that result in a workers' compensation case.
If an employer is notified in writing by the Bureau of Labor Statistics about having been selected to participate in a statistical survey, such employer, including small employers, and those in exempted SIC’s, must maintain a log and summary of all occupational injuries and illnesses for that year. The notification will contain the necessary form and instructions to comply with the survey requirements.
The Iowa Workers’ Compensation Act
The following is a summary of the recordkeeping and reporting responsibilities of employers under the Iowa Workers’ Compensation Act.
RECORDS AND REPORTS
Every employer shall keep a record of all injuries sustained by employees in the course of their employment resulting in incapacity for longer than one day. An employer with notice or knowledge of an injury which temporarily disables an employee for more than three (3) days or results in permanent total disability, permanent partial disability or death is required to file a report with the Workers' Compensation Commissioner, on State of Iowa Form No.
All books, records and payrolls of an employer are required to be open for inspection by the Workers' Compensation Commissioner for purposes of administration of the Iowa Workers’ Compensation Act.
The Workers' Compensation Commissioner may require an employer to appear and show cause why the employer should not be subject to a civil penalty of $100.00 per occurrence for failure to comply with the reporting or inspection requirements. Upon hearing, if the facts indicate, the commissioner may enter an order requiring payment of such penalty. Unless voluntarily paid, the commissioner may petition the district court for entry of judgment on the order. The employer’s insurance carrier shall be responsible in the same manner and to the same extent as the employer when a report of injury has been submitted to the employer’s insurance carrier and not filed by them with the Workers' Compensation Commissioner.
The employer is required to furnish to an employee, on request, one statement of earnings, wages or salary for the year preceding the injury. An employer may be subject to a civil penalty of $25.00 per offense for refusal to furnish such wage statement.
INSTRUCTIONS
An employer with notice or knowledge of an injury which temporarily disables an employee for more than THREE (3) days or results in permanent total disability, permanent partial disability or death is required to file a copy of this report with the Iowa DIVISION OF WORKERS' COMPENSATION within FOUR (4) days from such event when such injury is alleged by the employee to have been sustained in the course of the employee’s employment. A report to the Iowa DIVISION OF WORKERS' COMPENSATION is considered to also be a report to the Iowa DIVISION OF LABOR SERVICES. The Iowa DIVISION OF WORKERS' COMPENSATION shall forward this report to the Iowa Division of Labor Services. Employers should also report ALL injuries to their insurance carrier. ALL REPORTS MUST BE FILLED IN COMPLETELY AND
SIGNED. PLEASE TYPE OR PRINT LEGIBLY.
This form contains all items requested on OSHA form No 101, “Supplementary Record of Occupational Injuries and Illness.”
THE INFORMATION PROVIDED WILL BE OPEN FOR PUBLIC INSPECTION UNDER Iowa Code § 22.11.
Iowa Form
Document Specifics
| Fact Name | Detail |
|---|---|
| Governing Law | The form is governed by the Iowa Occupational Safety and Health Act and the Iowa Workers’ Compensation Act. |
| Primary Use | This form is used to report an injury or illness related to work in the jurisdiction of Iowa. |
| Submission Office | It must be mailed to the Division of Workers' Compensation, State of Iowa Division of Labor Services. |
| Comprehensive Reporting | The form requires detailed information about the claimant, employer, insurance policy, and the specifics of the injury or illness. |
| Employer Responsibilities | Employers are responsible for keeping records of occupational injuries and illnesses, requiring detailed logging and retention for 5 years. |
| Claim Administrator Role | Details about the claim administrator and the insurance carrier (if different) are critical components of the report. |
| Employee Information | Includes comprehensive personal and employment-related information, including injury/illness specifics and treatment. |
| Report Timing | An employer with notice of a disabling injury must file the report within four days from the event when it is alleged to have occurred during employment. |
| Incident Details | The form records specifics about the time, nature, and cause of the injury or illness, along with initial treatment details. |
| Legal Obligations | Failure to comply with reporting or inspection requirements can result in penalties, emphasizing the importance of accurate and timely filing. |
Guide to Writing First Report Of Injury Or Illness
Filling out the First Report of Injury or Illness is a crucial step following a workplace incident. This document ensures that the incident is officially recorded and sets the groundwork for an insurance claim under workers' compensation laws. To ensure clarity and completeness, follow these step-by-step instructions carefully. Your diligence not only facilitates a smoother claims process but also supports timely and fair compensation for the injured employee.
- Start with the Jurisdiction Code at the top of the form. Enter the code that corresponds to the state where the incident occurred.
- Fill in the Jurisdiction Claim Number if known; otherwise, leave it blank for the claim administrator to complete.
- Under CLAIM, provide the Claim Administrator Name, their Business Insurer Name if different, Phone Number, and Mailing Address including city, state, and postal code.
- Include the Claim Administrator Claim Number and both the Insurer FEIN and Claim Administrator FEIN.
- Detail the Claim Type Code as per the guidelines provided by the state or insurance carrier.
- In the EMPLOYER section, enter the Employer Name, FEIN, and Insured Report Number.
- Specify the Employer Type Code, and provide both the physical and mailing addresses including city, state, and postal code.
- Fill in the Industry Code, the Insured Location Number, and the Employer UI Number.
- Describe the Nature of Business, and provide the Employer Contact Name and Business Phone Number.
- For POLICY information, enter the Insured Name (or parent company), its FEIN, and Postal Code.
- Input the Policy/Contract Number, Coverage Effective and Expiration Dates, and the Self Insurance License/Certificate Number.
- Under EMPLOYEE, write the employee's full name, Date of Birth, and Gender.
- Check the appropriate box for the employee's Tax Filing Status and Marital Status.
- Input the Date of Hire, the employee's address, their Employment Status, ID Numbers (if applicable), and the Occupation Description.
- Record the employee's Educational Level and whether they authorize release of medical records and Social Security Number.
- For WAGE information, fill in the employee's Average Wage, select the payment frequency, and provide details on full wages paid for the date of injury.
- Detail the Date of Injury, the nature of the injury, when the employer and claim administrator were first informed, and the last day worked.
- Describe the ACCIDENT/INJURY, including the part(s) of body affected, whether there was a pre-existing disability, the premises code, and the event that caused the injury.
- In the MEDICAL section, indicate the initial treatment code, medical provider details, and whether future medical treatment or lost time is anticipated.
- Finally, the Preparer’s Name & Title, Company Name, and Phone Number must be filled in at the bottom of the form, along with the Date.
- Ensure all information is correct and complete before signing the form. Mail it to the address specified for the DIVISION OF WORKERS' COMPENSATION in the jurisdiction of the incident.
Accuracy and promptness are key when completing this form. A thorough and timely report not only complies with legal requirements but also ensures that the employee receives the necessary care and support. With the report filed, focus shifts to the claims process where decisions on compensation and medical coverage will be made based on the information provided.
Understanding First Report Of Injury Or Illness
FAQs about the First Report of Injury or Illness Form
When it comes to navigating the complexities of workers’ compensation, understanding the First Report of Injury or Illness form is essential. This document serves as the initial step in the claims process, providing essential information about the workplace incident. Here are some common questions answered to help guide you through this important process:
- What is the First Report of Injury or Illness form?
- Who needs to fill out the First Report of Injury or Illness form?
- When should the First Report of Injury or Illness form be submitted?
- What happens after the First Report of Injury or Illness form is submitted?
Upon submission, the form is reviewed by the workers' compensation board and/or the insurance carrier. This kicks off the claims process, which includes an evaluation of the injury or illness to determine if it’s work-related and the extent of any benefits the employee is entitled to.
The employee will receive instructions on how to seek medical treatment, if not already done, and information about potential benefits. This can include coverage for medical expenses, rehabilitation costs, and lost wages.
An investigation might be initiated, especially if there are discrepancies or if the incident is of a serious nature. Both the employer and the employee may be asked to provide additional information.
This form is a crucial document in the workers’ compensation process. It records detailed information about an employee's work-related injury or illness. It's designed to ensure quick and accurate communication with the workers' compensation board, insurance companies, and other relevant entities. The form includes sections about the injured or ill worker, the employer, the insurer, and details of the incident, such as how, when, and where the injury or illness occurred.
In most cases, the responsibility falls on the employer. Upon learning about an injury or illness, the employer must complete and submit this form to their workers' compensation insurance provider. It’s important for the accuracy of the claim that the information provided is as detailed and precise as possible, covering everything from the nature of the injury or illness to the circumstances under which it occurred.
Time frames for submission can vary by jurisdiction, but it’s generally required that the form be submitted within a few days after the employer is made aware of the injury or illness. It’s pertinent to check with your local workers' compensation board or insurance carrier for specific deadlines to ensure compliance and expedite the claims process.
It's essential to approach this form with thoroughness, understanding its importance in the workers’ compensation process. Prompt and accurate completion helps ensure that injured or ill employees receive the support and benefits they need during their recovery.
Common mistakes
When filling out the First Report of Injury or Illness form, individuals often make mistakes that could affect the processing or accuracy of the report. Understanding these common errors can help in filling out the form correctly and efficiently. Below are nine common mistakes:
- Incorrect or incomplete Jurisdiction Code entry – This code is crucial for directing the form to the appropriate managing entity.
- Failing to provide the complete details of the Claim Administrator – This includes the Claim Administrator Name, Business Insurer Name if different, ADMIN Phone Number, and Mailing Address, City, State, & Postal Code. Accurate information ensures proper communication and handling of the claim.
- Omitting Employer and Insured Information sections – Including all relevant data such as Employer Name, Employer FEIN, Insured Name, Policy/Contract Number, and Coverage dates are mandatory for claim processing.
- Neglecting to specify the employee's information correctly – Errors in the Employee's Name, Date of Birth, Gender, Educational Level, Marital Status, Employment Status, and Contact Information can lead to delays or incorrect processing of the claim.
- Leaving out details about the wage – Information regarding the basis of the employee's wage (e.g., hourly, daily, weekly) and whether the full wages were paid for the date of injury is important for determining compensation.
- Failure to accurately describe the nature of the injury or illness, including the Part(s) of body affected – This information is essential for assessing the claim and the benefits eligibility.
- Not providing a clear Accident/Injury Description – Including how, where, and when the injury or illness occurred helps in understanding the circumstances and potential coverage.
- Omitting information on initial treatment and medical provider – This includes not indicating the type of initial treatment received or failing to name the initial medical provider, which is important for medical claim processing.
- Incorrect or missing Preparer information – The individual completing the form must provide their Name, Title, Company Name, and Phone Number. This ensures accountability and provides a contact point for any follow-up needed.
In addition to these common mistakes, it's also crucial to submit the form within the stipulated timeframe to ensure timely processing and avoid penalties. Ensuring accuracy and completeness when filling out the First Report of Injury or Illness form is essential for a smooth claim process.
Documents used along the form
When dealing with workplace injuries and navigating the complexities of workers' compensation claims, several key forms and documents are often required in tandem with the First Report of Injury or Illness form. These documents play a crucial role in ensuring that all necessary details are accurately recorded, claims are processed efficiently, and employees receive the appropriate support and compensation they deserve. Understanding these forms can be pivotal for both employers and employees alike.
- OSHA Form 300 (Log of Work-Related Injuries and Illnesses): This form is a comprehensive log that employers must maintain to record significant work-related injuries and illnesses. It details each incident's nature, classification, and outcome, providing a year-long overview of workplace safety.
- OSHA Form 301 (Injury and Illness Incident Report): This document serves as an in-depth report for each individual recordable injury or illness listed on OSHA Form 300. It collects detailed information about the circumstances leading up to the injury or illness, including where and how it occurred.
- Wage Statement Form: Often required in workers' compensation claims, this document outlines an injured employee's earnings prior to the incident. It's crucial for calculating compensation benefits, especially when dealing with lost wages.
- Authorized Treating Physician Report: A critical document where the designated physician provides details on the employee's diagnosis, treatment plan, and any recommended work restrictions or accommodations. This report is vital for determining an employee's eligibility for workers' compensation benefits.
- Employee’s Claim for Workers’ Compensation Benefits: This form is filed by the employee or their representative to officially claim workers' compensation benefits. It includes personal information, details of the injury or illness, and the type of benefits being requested.
Navigating the aftermath of a workplace injury involves numerous steps and documentation to ensure the well-being of employees and compliance with legal requirements. From initial injury logs to detailed medical reports and benefit claims, each document plays its part in the intricate process of workers' compensation. By understanding the purpose and significance of these documents, both employers and employees can better navigate the process towards a resolution that supports recovery and fairness.
Similar forms
The Workers' Compensation Claim Form shares similarities with the First Report of Injury or Illness form, as both documents serve as initial notifications of a workplace injury or illness. The Workers' Compensation Claim Form is typically used by employees to file a claim for benefits following a work-related injury or illness, detailing similar information such as personal details, employment information, and the nature of the injury or illness. This form is crucial for initiating the claim process with an employer's workers' compensation insurance.
The OSHA 300 Log is another document related to the First Report of Injury or Illness form. While the First Report provides detailed information about a single incident, the OSHA 300 Log is a record-keeping form used to summarize work-related injuries and illnesses noted throughout the year. Employers must enter each injury or illness that meets OSHA's recording criteria into this log, making it a comprehensive record that supports workplace safety analyses and tracking over time.
Similar to the First Report of Injury or Illness form, the Incident Report Form is used within organizations to document any incident that occurs, not limited to work-related injuries. This can include property damage, security breaches, or any situation needing investigation. Both forms collect detailed information about the incident, including the date, time, individuals involved, and a description of the event, but the Incident Report Form may be used in a broader array of contexts beyond just injuries or illnesses.
The Employer's Report of Industrial Injury form serves a parallel function to the First Report of Injury or Illness form, specifically for reporting work-related injuries or illnesses for insurance and regulatory purposes. This document is typically submitted to the state labor department or a workers' compensation board and includes details about the injured employee, their employment, and the accident. It plays a vital role in the workers' compensation system by officially documenting the incident for potential benefits evaluation.
The Disability Claim Form is akin to the First Report of Injury or Illness form, mainly used when an employee seeks disability benefits due to a non-occupational illness or injury. Though its focus is broader, encompassing disabilities that are not work-related, the form still requires detailed information about the illness or injury, mirroring the First Report's structure in capturing the nature of the condition and its impact on the employee's ability to work.
The Accident Investigation Report, like the First Report of Injury or Illness form, is compiled following a specific incident, aiming to analyze the event's causes and prevent future occurrences. This report extends beyond mere documentation, delving into the accident's mechanics, contributing factors, and recommending safety measures. Whereas the First Report is designed for immediate notification and record-keeping, the Accident Investigation Report focuses on analysis and prevention.
The Near Miss Report documents incidents that could have resulted in injury, illness, or damage but did not, closely relating to the proactive safety intention behind the First Report of Injury or Illness form. By documenting near misses, organizations can identify and mitigate risks before they lead to actual harm. Although the outcomes differ from the incidents recorded on the First Report, the goal of preventing future incidents aligns them closely.
Last, the Employee's Claim for Workers' Compensation Benefits form is directly related to the First Report of Injury or Illness form in the continuum of workers' compensation processes. After an injury or illness is first reported, this claim form is the next step for employees seeking compensation for medical treatment, lost wages, or other support due to a workplace injury or illness. It builds upon the initial report's data, requiring further specifics about the impact of the injury or illness on the employee's work and life.
Dos and Don'ts
When completing the First Report of Injury or Illness form, it is crucial to ensure the accuracy and completeness of the information provided. Below are eight key recommendations to help guide you through this process:
- Do verify the spelling of all names and accuracy of all dates, such as the date of injury and the employee's date of birth, to avoid any discrepancies.
- Don't leave any required fields incomplete. If a section does not apply, mark it as "N/A" (Not Applicable) instead of leaving it blank.
- Do provide detailed descriptions where required, especially in the section that asks for the nature of the injury or illness and the description of the accident. Be specific to ensure a clear understanding of the incident.
- Don't guess on information. If you're unsure about specific details, such as the exact time of injury or the ICD Diagnostic Code, it's better to confirm these details before submitting the form.
- Do review the entire form for accuracy and completeness before submission. Double-check names, identification numbers, and contact information for errors.
- Don't disregard the employee's privacy. Ensure that sensitive information, such as Social Security numbers and medical records, is handled confidentially and in accordance with privacy laws and regulations.
- Do use the space provided on the form efficiently. If additional space is needed for descriptions or explanations, attach a separate sheet of paper and clearly indicate which section the information refers to.
- Don't hesitate to contact the relevant workers' compensation board or insurance carrier for guidance if you encounter any uncertainties or questions while filling out the form.
By following these recommendations, you can help streamline the process of reporting an injury or illness, ensuring that the information provided is both accurate and complete. This not only aids in the efficient processing of the claim but also supports a clear and fair assessment of the incident for all parties involved.
Misconceptions
There are several misconceptions about the First Report Of Injury Or Illness form that if clarified could help both employers and employees navigate the complexities of workers' compensation claims more effectively. This list aims to dispel some of the common misunderstandings surrounding the form.
Misconception 1: The form is only necessary for severe injuries. Actually, the form should be completed for any injury or illness that arises out of the course of employment, regardless of its severity. This ensures that all incidents are properly documented right from the start.
Misconception 2: Employees are responsible for filling out the form. In fact, it is the employer's responsibility to complete and file the First Report Of Injury Or Illness form, not the employee's. However, employees should provide all necessary information to their employer.
Misconception 3: The form must be filed with the state immediately after an injury occurs. While timely reporting is essential, the specific timeframe to submit the form varies by state. It's vital to understand the local jurisdiction's requirements to ensure compliance.
Misconception 4: Only physical injuries need to be reported. The form should also be used for illnesses that are related to the job, including those caused by exposure to harmful substances or environments.
Misconception 5: Filing the form initiates a claim for workers' compensation benefits. Submitting the form is a critical step in the process, but it alone does not start a claim. Employees must follow additional steps to file a claim.
Misconception 6: All sections of the form must be filled out for it to be accepted. While it is important to provide comprehensive information, some sections may not apply to every incident. Employers should complete the form to the best of their ability, ensuring to fill out all relevant sections.
Misconception 7: The form is the only documentation needed for a workers' compensation claim. The First Report Of Injury Or Illness form is just the initial step. Additional documentation, such as medical records and witness statements, may be required to support the claim.
Misconception 8: The form is only used for workers' compensation purposes. While its primary purpose is for workers' compensation, the information provided can also be useful for improving workplace safety and preventing future injuries.
Misconception 9: If a business has no employees, it does not need to worry about the form. Businesses that use contractors or non-traditional employees may still need to report certain incidents, depending on state laws and the specifics of the working arrangement.
Misconception 10: A lack of immediate symptoms means an injury doesn't need to be reported. Sometimes, the effects of an injury or illness are not immediately apparent. It is better to report any incident that could potentially result in a claim later on.
Understanding these misconceptions is critical for both employers and employees to ensure that the First Report Of Injury Or Illness form is used correctly and effectively. When in doubt, seek clarification to avoid potential complications in the workers' compensation process.
Key takeaways
Filling out the First Report Of Injury Or Illness form accurately and promptly is crucial for employers in managing workers' compensation claims. It initiates the claim process by documenting the injury or illness an employee sustains at work. Here are five key takeaways regarding the completion and use of this form:
- Timeliness is critical: Employers must complete and submit the form within specific timeframes mandated by their jurisdiction. For instance, in Iowa, an employer with notice or knowledge of an injury resulting in more than three days of temporary disability or resulting in permanent total or partial disability, or death, must file the report within four days of the event. Filing within these timeframes ensures compliance with state regulations and facilitates the timely processing of the worker's compensation claim.
- Accuracy matters: When filling out the form, it's essential to provide accurate and comprehensive details about the injured or ill employee, the nature and circumstances of the injury or illness, including the date, time, and cause, as well as the specific parts of the body affected. Accurate documentation helps prevent delays and ensures that the employee receives the appropriate benefits.
- Comprehensive documentation: The First Report Of Injury Or Illness form requires detailed information on the employer, the policy under which the claim is filed, and the specific circumstances of the accident or illness, including any witnesses and the initial medical treatment. Gathering this information thoroughly supports the claim's evaluation process, helping insurers and medical providers understand the incident and its impact on the employee.
- Privacy considerations: The form includes sections that may involve sensitive employee information, such as social security numbers and medical records. It is crucial to handle these sections with care, respecting privacy laws and ensuring that the information is shared only with authorized parties involved in the workers' compensation claim process.
- Legal and regulatory compliance: Completing and submitting the First Report Of Injury Or Illness form is not just about initiating the claim process. It also helps employers comply with state workers' compensation laws and occupational safety and health regulations. Non-compliance can result in penalties, fines, and other legal implications. Additionally, maintaining accurate records and submitting them as required supports employers in case of audits or disputes.
Properly managing the First Report Of Injury Or Illness form is a fundamental part of handling workers' compensation claims, ensuring both compliance with the law and the well-being of employees.
Popular PDF Documents
2253 Form - IRS form 2553 must be filed by a corporation or an entity eligible to be classified as a corporation that seeks to be taxed as an S corporation.
IRS 1041 - It is also used to claim deductions for expenses like trustee fees, attorney fees, and administration costs.
Uncollected Social Security and Medicare Tax on Wages - Submitting Form 8919 can have implications for future employment benefits, including unemployment and Social Security benefits.