Get First Report Of Injury Florida Form
In the state of Florida, when an employee sustains an injury or falls ill due to their work environment or activities, it is crucial for the incident to be officially recorded and processed through the First Report of Injury or Illness form, provided by the Florida Department of Financial Services Division of Workers' Compensation. This document serves as a foundational piece in the claims process, requiring detailed input about the employee involved, including their personal and employment details, the nature and specifics of the injury or illness sustained, and a thorough description of the accident or circumstances leading to the injury. The form also gathers information on the employer, including the company's name and policy number, signaling the commencement of an official claim. It is designed to facilitate the prompt reporting of such incidents to ensure timely evaluation and provision of applicable benefits. Additionally, the form plays a crucial role in maintaining an accurate and comprehensive record for the Division of Workers' Compensation, aiding in the administration and oversight of claims. Drawing upon the mandatory reporting requirements, this document underscores the importance of transparency and promptness in addressing workplace injuries, emphasizing the rights and responsibilities of both employers and employees in the aftermath of workplace incidents.
First Report Of Injury Florida Example
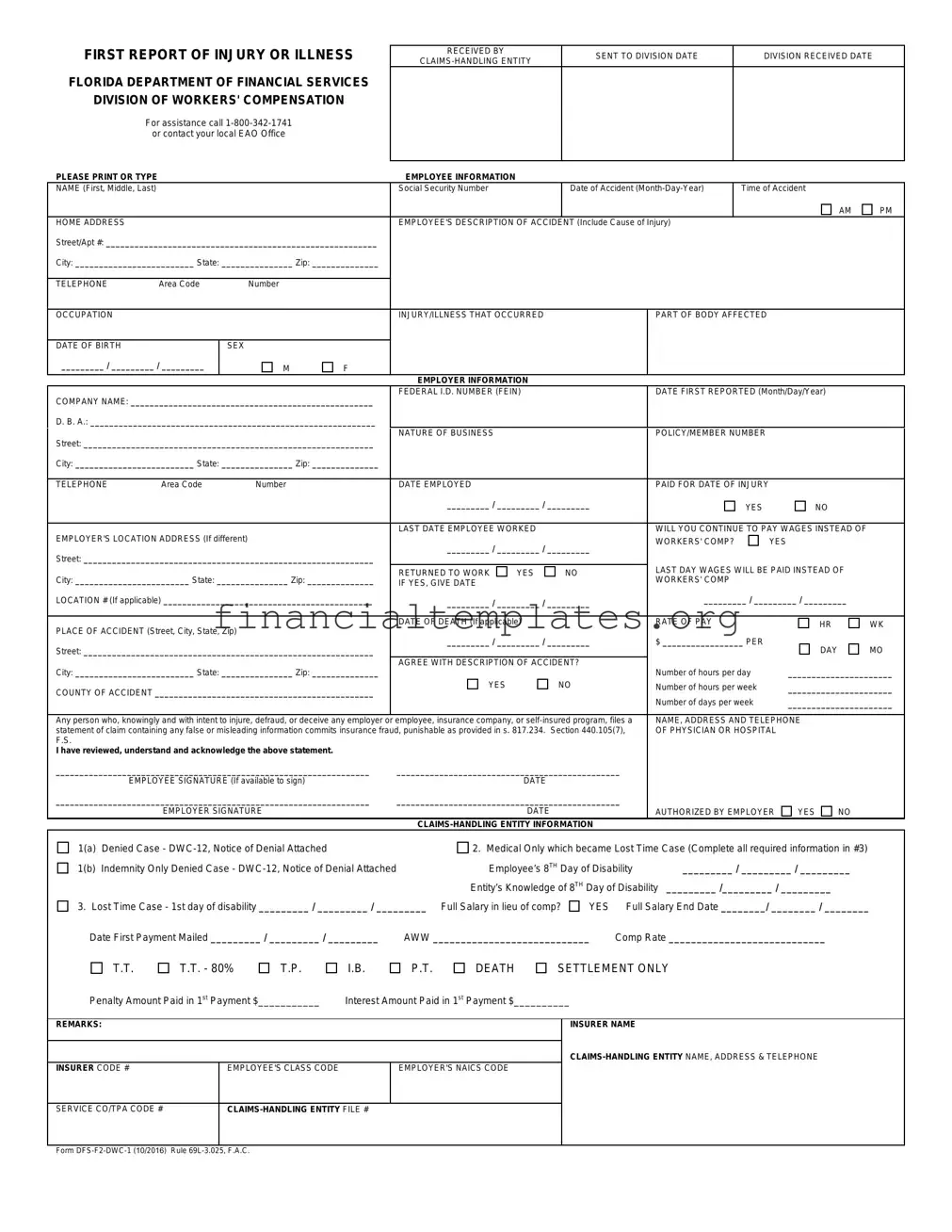
FIRST REPORT OF INJURY OR ILLNESS
FLORIDA DEPARTMENT OF FINANCIAL SERVICES
DIVISION OF WORKERS' COMPENSATION
For assistance call
PLEASE PRINT OR TYPE
RECEIVED BY |
SENT TO DIVISION DATE |
DIVISION RECEIVED DATE |
|
|
|
||
|
|
|
EMPLOYEE INFORMATION
NAME (First, Middle, Last) |
|
|
|
Social Security Number |
|
|
Date of Accident |
|
Time of Accident |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
HOME ADDRESS |
|
|
|
EMPLOYEE'S DESCRIPTION OF ACCIDENT (Include Cause of Injury) |
|
|
|
|
|||||
Street/Apt #: _________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
Area Code |
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
OCCUPATION |
|
|
|
INJURY/ILLNESS THAT OCCURRED |
|
|
PART OF BODY AFFECTED |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
SEX |
|
|
|
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER INFORMATION |
|
|
|
|
|
|
|
|
|
COMPANY NAME: ___________________________________________________ |
FEDERAL I.D. NUMBER (FEIN) |
|
|
DATE FIRST REPORTED (Month/Day/Year) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||
D. B. A.: ____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
Street: _____________________________________________________________ |
NATURE OF BUSINESS |
|
|
|
POLICY/MEMBER NUMBER |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
TELEPHONE |
Area Code |
Number |
|
DATE EMPLOYED |
|
|
|
PAID FOR DATE OF INJURY |
|
|
|
||
|
|
|
|
_________ / _________ / _________ |
|
|
YES |
|
NO |
|
|||
|
|
|
|
|
|
|
|
|
|
||||
EMPLOYER'S LOCATION ADDRESS (If different) |
|
LAST DATE EMPLOYEE WORKED |
|
|
WILL YOU CONTINUE TO PAY WAGES INSTEAD OF |
|
|||||||
|
_________ / _________ / _________ |
WORKERS' COMP? |
|
YES |
|
||||||||
|
|
|
|
|
|
||||||||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|||||||
|
|
|
|
LAST DAY WAGES WILL BE PAID INSTEAD OF |
|
||||||||
|
|
|
|
RETURNED TO WORK |
YES |
|
NO |
|
|||||
City: ________________________ State: _______________ Zip: ______________ |
|
WORKERS' COMP |
|
|
|
|
|||||||
IF YES, GIVE DATE |
|
|
|
|
|
|
|
||||||
LOCATION # (If applicable) ____________________________________________ |
_________ / _________ / _________ |
_________ / _________ / _________ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
RATE OF PAY |
|
|
|
|
||
PLACE OF ACCIDENT (Street, City, State, Zip) |
|
DATE OF DEATH (If applicable) |
|
|
|
|
HR |
WK |
|||||
|
|
|
|
|
|
|
|
|
|||||
|
_________ / _________ / _________ |
$ _________________ PER |
|
|
|
||||||||
Street: _____________________________________________________________ |
|
DAY |
MO |
||||||||||
|
|
|
|
|
|
|
|
||||||
City: _________________________ State: _______________ Zip: ______________ |
AGREE WITH DESCRIPTION OF ACCIDENT? |
Number of hours per day |
______________________ |
||||||||||
|
|
|
|
||||||||||
COUNTY OF ACCIDENT ______________________________________________ |
YES |
|
NO |
Number of hours per week |
______________________ |
||||||||
|
|
|
|
Number of days per week |
______________________ |
||||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|||||||||
Any person who, knowingly and with intent to injure, defraud, or deceive any employer or |
employee, insurance company, or |
NAME, ADDRESS AND TELEPHONE |
|
||||||||||
statement of claim containing any false or misleading information commits insurance fraud, punishable as provided in s. 817.234. Section 440.105(7), |
OF PHYSICIAN OR HOSPITAL |
|
|||||||||||
F.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
I have reviewed, understand and acknowledge the above statement.
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYEE SIGNATURE (If available to sign) |
DATE |
|
|
|
|
|
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYER SIGNATURE |
DATE |
|
AUTHORIZED BY EMPLOYER |
YES |
NO |
|
|
|
|
|
|
|
||
1(a) |
Denied Case - |
2. Medical Only which became Lost Time Case (Complete all required information in #3) |
|||||
1(b) |
Indemnity Only Denied Case - |
Employee’s 8TH Day of Disability |
_________ / _________ / _________ |
||||
|
|
Entity’s Knowledge of 8TH Day of Disability |
_________ /_________ / _________ |
|
|||
3. Lost Time Case - 1st day of disability _________ / _________ / _________ Full Salary in lieu of comp? |
YES |
Full Salary End Date ________/ ________ / ________ |
|||||
Date First Payment Mailed _________ / _________ / _________ |
AWW ____________________________ |
Comp Rate ____________________________ |
|
||||
T.T.
T.T. - 80%
T.P.
I.B.
P.T.
DEATH
SETTLEMENT ONLY
Penalty Amount Paid in 1st Payment $___________ |
Interest Amount Paid in 1st Payment $__________ |
REMARKS:
INSURER CODE # |
EMPLOYEE'S CLASS CODE |
EMPLOYER'S NAICS CODE |
|
|
|
INSURER NAME
SERVICE CO/TPA CODE #
Form
The collection of the social security number on this form is specifically authorized by Section 440.185(2), Florida Statutes. The social security number will be used as a unique identifier in Division of Workers' Compensation database systems for individuals who have claimed benefits under Chapter 440, Florida Statutes. It will also be used to identify information and documents in those database systems regarding individuals who have claimed benefits under Chapter 440, Florida Statutes, for internal agency tracking purposes and for purposes of responding to both public records requests and subpoenas that require production of specified documents. The social security number may also be used for any other purpose specifically required or authorized by state or federal law.
Document Specifics
| Fact Name | Detail |
|---|---|
| Form Designation | The official name is the First Report Of Injury Or Illness Florida. |
| Governing Body | The form is governed by the Florida Department of Financial Services, Division of Workers' Compensation. |
| Assistance Information | For assistance, individuals can call 1-800-342-1741 or contact their local EAO Office. |
| Legal Framework | The form is supported by Chapter 440, Florida Statutes, specifically mentioning Sections 440.185(2) and 440.105(7) concerning the use of social security numbers and insurance fraud, respectively. |
| Purpose and Usage | The form's purpose is to report injuries or illnesses associated with work, detailing the claimant's and employer's information, accident description, and compensation details. |
Guide to Writing First Report Of Injury Florida
Filling out the First Report of Injury or Illness form is an essential step for documenting a workplace injury or illness in Florida. It allows workers to report any injury or illness that occurred as a result of their job to the Florida Department of Financial Services, Division of Workers' Compensation. This documentation is crucial for processing workers' compensation claims effectively. Here's how to accurately complete the form:
- At the top of the form, where it says "RECEIVED BY" and "SENT TO DIVISION," leave these sections blank if you are the one initially filling out the form.
- Under "EMPLOYEE INFORMATION," start by entering the full name (First, Middle, Last) of the injured or ill employee.
- Enter the Social Security Number, and fill in the exact Date of Accident, including selecting AM or PM for the Time of Accident.
- Provide the complete Home Address including Street/Apt #, City, State, and Zip. Include the employee's Telephone number with the area code.
- In the section titled "EMPLOYEE'S DESCRIPTION OF ACCIDENT," clearly describe how the accident happened and what caused the injury or illness. Be sure to include specifics about the injury/illness and what part of the body was affected.
- Fill in the Date of Birth, select Sex (M for male, F for female).
- For "EMPLOYER INFORMATION," write the company name and include the Federal I.D. Number (FEIN).
- Detail the Date First Reported, Nature of Business, and Policy/Member Number. Provide the employer's address, including Street, City, State, Zip, and Telephone number.
- Indicate the Date Employed, if the employee was Paid for Date of Injury by selecting Yes or No, and fill in the Employer's Location Address if it differs.
- Note the Last Date Employee Worked and whether wages will continue to be paid instead of workers' compensation benefits.
- Mark if the employee has Returned to Work and the Rate of Pay, along with the Place of Accident (including full address).
- If applicable, provide the Date of Death.
- Under the section requiring information about the Physician or Hospital, write the name, address, and telephone number of the first medical provider that treated the employee after the accident.
- The employee and employer must sign and date the bottom of the form, verifying all provided information is accurate.
- Finally, complete the "CLAIMS-HANDLING ENTITY INFORMATION" section based on the current status of the case and the actions taken by the claims-handling entity.
After completing the form with accurate and concise information, review it to ensure no sections were missed or filled out incorrectly. This form should then be submitted according to the instructions provided by the Florida Department of Financial Services or your workplace's standard protocol for workers' compensation claims. Timely and accurate submission is crucial to ensure the proper processing of the claim.
Understanding First Report Of Injury Florida
What is the First Report of Injury or Illness form in Florida?
The First Report of Injury or Illness form, known officially as DFS-F2-DWC-1, is a document required by the Florida Department of Financial Services, Division of Workers' Compensation. It serves as the initial notification of an employee's work-related injury or illness. Employers or claims-handling entities must complete and submit this form to document the incident details, including the employee's personal information, a description of the accident, the nature of the injury or illness, and employer information. This form is crucial for initiating a workers' compensation claim in Florida.
When should the First Report of Injury or Illness form be filed?
This form should be filed as soon as possible after the employee reports an injury or illness related to their work. The State of Florida requires that this notification be made within seven days of becoming aware of the injury or illness. Delay in filing the form can result in penalties and delays in the injured employee receiving necessary benefits.
Who is responsible for filing the First Report of Injury or Illness form?
The employer is primarily responsible for filing the First Report of Injury or Illness form. However, in many cases, the responsibility to fill out and submit the form is delegated to the claims-handling entity, such as an insurance company or third-party administrator, that manages workers' compensation claims on behalf of the employer. It's important for employers to ensure that the form is properly and promptly filed to uphold their compliance with state regulations.
What information is needed to complete the form?
To complete the First Report of Injury or Illness form, the following information is required:
- Employee information, including full name, social security number, date of birth, home address, and occupation;
- Detailed description of the accident and injury or illness, including the date, time, and location of the accident, as well as the part of the body affected;
- Employer information, such as company name, federal ID number, and policy/member number;
- Initial treatment information, including the name, address, and telephone number of the physician or hospital providing care.
What happens after the First Report of Injury or Illness form is filed?
Once the First Report of Injury or Illness form is filed, it triggers the workers' compensation process. The claims-handling entity will review the claim and determine eligibility for benefits, which may include medical treatment, wage replacement, and other necessary supports. The employee may be contacted for further information or to provide additional documentation related to their injury or illness. Timely and accurate filing of this form is essential to ensure the injured employee receives all appropriate benefits without unnecessary delays.
Common mistakes
Completing the First Report of Injury or Illness form for the Florida Department of Financial Services, Division of Workers' Compensation, is a critical process that requires accuracy to ensure prompt and proper handling of a worker's compensation claim. Below are ten common mistakes people make when filling out this document:
Not providing complete employee information, including full name, social security number, and contact details. This is crucial for identifying the claim and ensuring the individual receives the appropriate benefits.
Failing to accurately detail the date and time of the accident. Precise information helps in the investigation and processing of the claim.
Omitting or providing vague descriptions of the accident and cause of injury. A clear account of the events leading to the injury or illness is essential for determining compensability.
Leaving out information on the part of the body affected. Identifying the specific area injured is necessary for assessing the claim and the type of medical treatment required.
Incorrectly filling in employer information, such as the company name, FEIN, and policy number. This information ensures that the claim is attributed to the correct employer and their insurance policy.
Not specifying if full wages will be paid instead of workers' compensation, or failing to provide the last day wages will be paid. This affects the calculation of benefits.
Forgetting to indicate whether the employee returned to work. This information helps in adjusting the claim and determining ongoing eligibility for benefits.
Misidentifying the place of accident. Accurate location details are necessary for verifying the claim, especially if the injury occurred outside of the usual place of employment.
Signature omissions: Not having the form signed by both the employee and the employer or authorized representative can result in processing delays. Signatures validate the authenticity of the claim.
Leaving the physician or hospital information blank or incomplete. Initial medical provider information is critical for follow-up and verification of medical treatment related to the claim.
Avoiding these mistakes can expedite the claims process, ensuring that injured workers receive the support and benefits they are entitled to in a timely manner. It's worth double-checking each section of the form for completeness and accuracy before submission.
Documents used along the form
When filing a First Report of Injury or Illness with the Florida Department of Financial Services, Division of Workers' Compensation, it is not uncommon for other forms and documents to be necessary. Each document serves a specific purpose in the workers' compensation claim process, facilitating efficient communication and decision-making among all parties involved. Below is an outline of nine forms and documents frequently used alongside the initial injury or illness report.
- DWC-12, Notice of Denial: This document is issued if the claims-handling entity decides to deny the claim. It explains the reasons for denial and outlines the employee's rights and next steps.
- DWC-3, Employer’s Wage Statement: This form is used to report the injured worker's wages to determine benefit rates. It helps ensure accurate calculation of compensation.
- DWC-25, Request for Authorization: Healthcare providers use this form to request authorization for treatment of the injured worker. It outlines proposed treatment plans and estimated costs.
- Employee's Claim for Workers' Compensation Benefits: This document is filled out by the injured employee if they need to claim benefits. It includes details of the injury and lost wages.
- Wage Statement for Exempt Employees: Similar to the DWC-3 form but specifically for employees exempt from regular workers' compensation coverage, such as certain executive officers.
- Mileage Reimbursement Form: Injured workers use this form to request reimbursement for travel expenses related to medical appointments, treatments, or pharmacy visits.
- Physician’s Report on Disability: A detailed report from the treating physician that describes the employee's current medical condition, ability to work, and anticipated return-to-work date.
- Release of Medical Records Authorization: This allows the employer or insurance carrier to obtain the injured worker’s medical records related to the injury or illness claim.
- Permanent Impairment Rating Form: Used when a physician determines that the injured employee has reached maximum medical improvement and assesses any permanent impairment resulting from the injury.
Understanding and completing these forms accurately is crucial in the process of reporting a workplace injury or illness in Florida. They ensure that all necessary information is collected for evaluating the claim, determining eligibility for benefits, and facilitating the injured employee's return to work when possible. It's recommended for employers and employees to familiarize themselves with these documents and seek clarification if needed.
Similar forms
The "Worker's Compensation Claim Form" is closely aligned with the First Report of Injury or Illness form in Florida. Both documents serve as the initial notice that an employee has been injured or has fallen ill due to their workplace environment or activities. The key purpose is to officially communicate with the relevant state department or workers' compensation insurance provider about the incident. They collect similar types of information, such as the employee's personal details, a description of the accident, injury or illness details, and employment information. However, each state might have specific fields or requirements based on local regulations.
The "Employee's Claim for Workers' Compensation Benefits" form mirrors the First Report of Injury form in its goal to initiate a workers' compensation claim. While the former is often filled out and submitted by the employee or their representative, the First Report of Injury is usually completed by the employer. Both forms gather detailed information about the incident, such as the date, time, and nature of the injury or illness, as well as the affected parts of the body. This parallel structure ensures all relevant details are captured to process the claim efficiently.
The "Employer's First Report of Occupational Injury or Illness" form presents another example of documentation similar to Florida's First Report of Injury or Illness form. Filed by employers to report an employee's work-related injury or illness, this form shares many characteristics, including collecting data on the employee's condition, the circumstances surrounding the incident, and the initial medical response. The primary aim of both forms is to start the workers' compensation process, ensuring that the claim is documented and that the employee receives the necessary support and benefits.
The "Notice of Employee's Injury or Death" form accompanies the First Report of Injury or Illness form in its functionality to inform relevant authorities and parties about a work-related injury or fatality. This notice plays a crucial role in the workers' compensation claim process, similar to the initial report form, by officially documenting the incident. It requires information on the injured or deceased worker, the employer, and details of the injury or death, underlining the severity and specifics of each case to facilitate appropriate actions and benefits.
Dos and Don'ts
When completing the First Report of Injury or Illness form for the Florida Department of Financial Services Division of Workers' Compensation, it is vital to ensure accuracy and completeness to facilitate the processing of your claim. Below are essential dos and don'ts to guide you through this process.
Things you should do:
- Ensure all information is printed or typed clearly to prevent any misunderstandings or processing delays.
- Provide accurate and complete details about the employee and employer, including full names, addresses, and contact information, to enable efficient communication.
- Include a thorough and precise description of the accident and the injury or illness that occurred, specifying the part of the body affected.
- Report the incident promptly, noting the exact date and time of the accident, to comply with reporting deadlines and facilitate timely claim processing.
- Verify that the employee's Social Security Number is included as it acts as a unique identifier in the Division of Workers' Compensation database systems.
- Review and acknowledge the information concerning insurance fraud on the form, underscoring the importance of providing truthful information.
Things you shouldn't do:
- Do not leave any required fields blank, as incomplete forms can lead to delays in processing or denial of the claim.
- Avoid providing ambiguous or vague descriptions of the accident or injury, as this can complicate understanding and verification of the claim.
- Do not guess information, especially regarding dates and times; inaccurate information can adversely affect the claim's outcome.
- Avoid neglecting to review the accuracy of all the provided information before submission to prevent errors and potential disputes.
- Do not fail to sign the form, as an unsigned report may not be processed until it is acknowledged by the required parties.
- Refrain from withholding information about previous or existing conditions that could be relevant to the current claim, as this could be construed as fraud.
Misconceptions
There are several misconceptions about the First Report of Injury or Illness (DWC-1) form in Florida that need clarifying to ensure both employers and employees handle workplace injuries and illnesses correctly. Below are five common misunderstandings:
- Misconception 1: The form is optional. In reality, this form is a critical component of the claims process in Florida for workplace injuries or illnesses. It's mandatory for employers to complete and file this form with their insurance carrier to initiate a worker's compensation claim.
- Misconception 2: Only serious injuries need to be reported. All workplace injuries or illnesses, regardless of their severity, should be reported using the DWC-1 form. This ensures that all incidents are documented, which can be crucial for later claims or investigations.
- Misconception 3: The employee is responsible for filing the form. The responsibility of completing and submitting the form actually falls on the employer, not the injured or ill employee. Though employees must report their injury or illness to their employer to kickstart the process.
- Misconception 4: There is no deadline for filing the form. The form must be filed by the employer with their workers' compensation insurance carrier as soon as possible, but no later than seven (7) days after learning of the injury or illness. Delayed filing can lead to penalties and complications in the claims process.
- Misconception 5: Filing the form admits liability. Submitting the DWC-1 form is a procedural step required under Florida law and does not necessarily admit employer liability for the injury or illness. It simply starts the process for potential compensation for the employee under the Workers' Compensation system.
Understanding the facts about the First Report of Injury or Illness form ensures that employers comply with legal obligations and that employees receive the benefits they're entitled to in a timely manner. It's crucial for both parties to understand their rights and responsibilities in the workers' compensation claims process.
Key takeaways
Filing a First Report of Injury or Illness (Form DFS-F2-DWC-1) with the Florida Department of Financial Services, Division of Workers' Compensation, is an essential step for both employers and employees following a workplace accident leading to injury or illness. Understanding how to correctly complete and utilize this form is crucial for ensuring that injured workers receive the benefits and support they are entitled to under Florida's workers' compensation laws. Here are key takeaways to bear in mind:
- The form requires detailed information about the employee, including their name, Social Security Number, home address, date of birth, sex, occupation, and a comprehensive description of the accident and injury or illness.
- Employer information is also crucial, including the company name, Federal Employer Identification Number (FEIN), the nature of business, policy/member number, and relevant employment dates.
- Accuracy in describing the accident, injury, or illness is paramount, as this information directly impacts the assessment and processing of the workers' compensation claim.
- If wages are continued instead of workers' compensation benefits, this must be clearly indicated, along with relevant dates and justification.
- The section related to the claims-handling entity information determines the progression of the claim, whether it's for medical only, lost time, or involves a denial of the case.
- Any attempt to provide false or misleading information on the First Report of Injury or Illness is considered insurance fraud, which is punishable under Florida law, highlighting the importance of honesty and accuracy when filling out the form.
- Contact information for the treating physician or hospital must be included, which aids in the verification of medical treatment and facilitates communication between healthcare providers and the insurance carrier or employer.
- The collection of the Social Security Number (SSN) on this form is specifically authorized and is used as a unique identifier within the Division of Workers' Compensation's database systems, underscoring the significance of this information for tracking and processing claims.
- Both the employee and the employer (or authorized representative) must sign the form, acknowledging the accuracy of the information provided and the understanding of legal liabilities related to false claims.
For additional assistance with filling out the First Report of Injury or Illness form, or for any questions related to workers' compensation claims in Florida, individuals are encouraged to call the provided assistance number or contact their local Employee Assistance Office (EAO).
Popular PDF Documents
Ach Form to Receive Payment - By requiring a signature, the form adds a level of verification and security to the electronic payment process.
Do I Need a Business License Report - Acquaint yourself with the need for detailed business information, from federal ID to social security numbers, for Tempe's records.