Get First Report Dfs F2 Dwc 1 Form
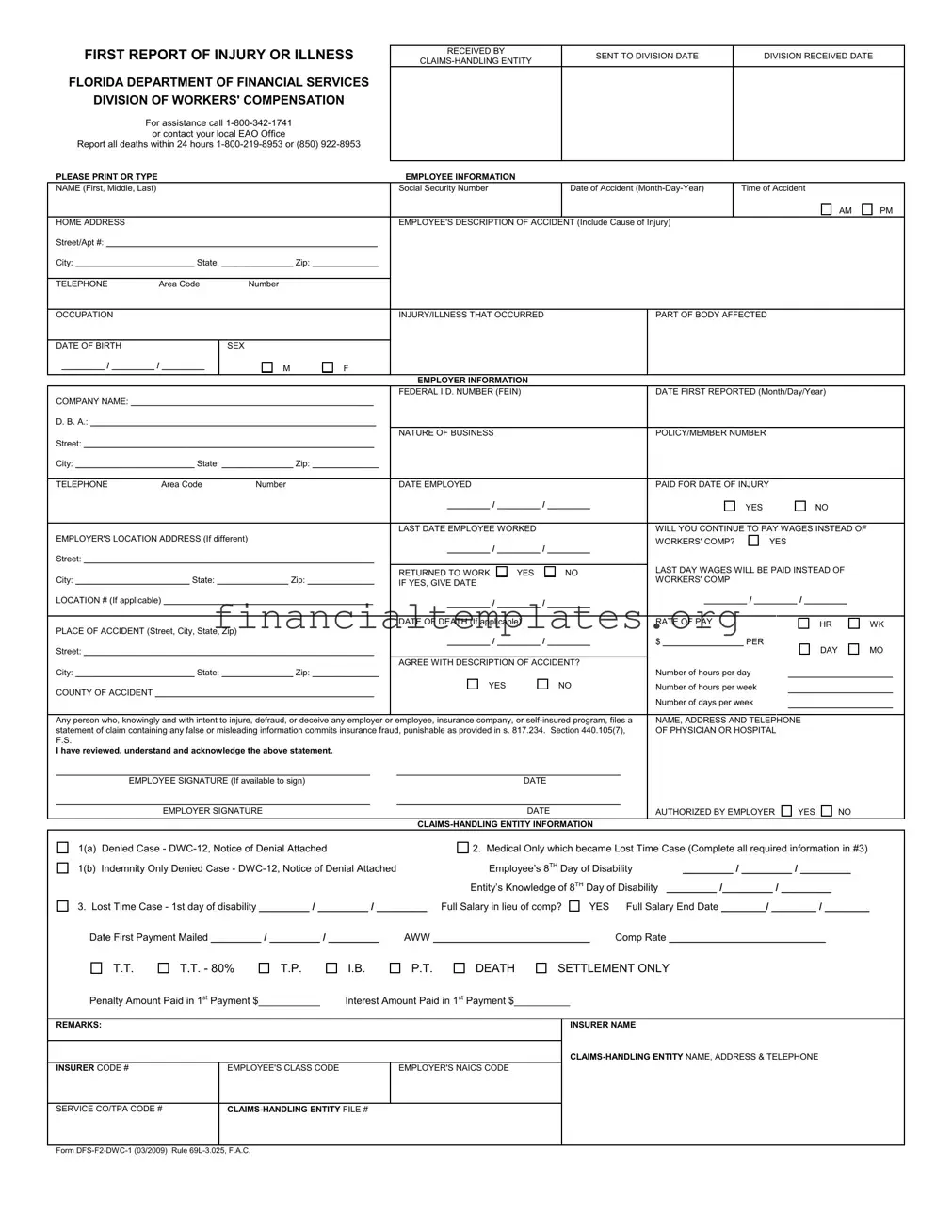
Dealing with workplace injuries or illnesses requires navigating a series of crucial steps to ensure both the wellbeing of the employee and the proper adherence to legal protocols. At the heart of this process in Florida is the First Report of Injury or Illness (DFS-F2-DWC-1 form), a document mandated by the Florida Department of Financial Services, Division of Workers' Compensation. This form initiates the formal reporting process for any workplace injury or illness, ensuring that employees receive the necessary assistance and the incident is officially documented. It requires detailed information about the employee, including their name, Social Security Number, home address, and the specifics of the accident, such as the date, time, and cause. It also gathers comprehensive data on the employer, including the Federal ID number, nature of business, and policy number. Beyond the basics, the form delves into the injury or illness itself, its severity, whether the employee has had to miss work, and if so, whether the employer intends to compensate the employee outside of workers' comp. Finally, the form acts as an initial checkpoint against fraudulent claims with a strict advisory against submitting false information. Each of these elements is designed to streamline the process of reporting, evaluating, and addressing workplace injuries and illnesses, safeguarding the interests of both the employee and employer within the state's legal framework.
First Report Dfs F2 Dwc 1 Example
FIRST REPORT OF INJURY OR ILLNESS
FLORIDA DEPARTMENT OF FINANCIAL SERVICES
DIVISION OF WORKERS' COMPENSATION
For assistance call
Report all deaths within 24 hours
PLEASE PRINT OR TYPE
RECEIVED BY |
SENT TO DIVISION DATE |
DIVISION RECEIVED DATE |
|
|
|
||
|
|
|
EMPLOYEE INFORMATION
NAME (First, Middle, Last) |
|
|
|
|
|
Social Security Number |
|
|
|
Date of Accident |
|
Time of Accident |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
HOME ADDRESS |
|
|
|
|
|
EMPLOYEE'S DESCRIPTION OF ACCIDENT (Include Cause of Injury) |
|
|
|
|
|||||||||
Street/Apt #: _________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
Area Code |
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
OCCUPATION |
|
|
|
|
|
INJURY/ILLNESS THAT OCCURRED |
|
|
|
|
PART OF BODY AFFECTED |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
SEX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
EMPLOYER INFORMATION |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
FEDERAL I.D. NUMBER (FEIN) |
|
|
|
|
DATE FIRST REPORTED (Month/Day/Year) |
|
|
|||||
COMPANY NAME: ___________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
D. B. A.: ____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
NATURE OF BUSINESS |
|
|
|
|
|
POLICY/MEMBER NUMBER |
|
|
|
|||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
TELEPHONE |
Area Code |
Number |
|
|
DATE EMPLOYED |
|
|
|
|
|
PAID FOR DATE OF INJURY |
|
|
|
|||||
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
|
|
|
YES |
NO |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
LAST DATE EMPLOYEE WORKED |
|
|
|
|
WILL YOU CONTINUE TO PAY WAGES INSTEAD OF |
|
||||||
EMPLOYER'S LOCATION ADDRESS (If different) |
|
|
|
|
|
|
|
|
|
|
WORKERS' COMP? |
YES |
|
|
|
||||
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
RETURNED TO WORK |
YES |
|
NO |
|
LAST DAY WAGES WILL BE PAID INSTEAD OF |
|
||||||
City: ________________________ State: _______________ Zip: ______________ |
|
|
|
WORKERS' COMP |
|
|
|
|
|||||||||||
|
IF YES, GIVE DATE |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
LOCATION # (If applicable) ____________________________________________ |
|
|
_________ / _________ / _________ |
|
_________ / _________ / _________ |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
DATE OF DEATH (If applicable) |
|
|
|
|
RATE OF PAY |
|
HR |
|
WK |
|||
PLACE OF ACCIDENT (Street, City, State, Zip) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
|
$ _________________ PER |
|
|
|
||||||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
DAY |
|
MO |
|||||
|
|
|
|
|
|
|
AGREE WITH DESCRIPTION OF ACCIDENT? |
|
|
|
|
|
|
|
|||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
Number of hours per day |
______________________ |
|||||||||
COUNTY OF ACCIDENT ______________________________________________ |
|
|
YES |
|
NO |
|
Number of hours per week |
______________________ |
|||||||||||
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number of days per week |
______________________ |
||||
|
|
|
|
|
|
||||||||||||||
Any person who, knowingly and with intent to injure, defraud, or deceive any employer or employee, insurance company, or |
NAME, ADDRESS AND TELEPHONE |
|
|
||||||||||||||||
statement of claim containing any false or misleading information commits insurance fraud, punishable as provided in s. 817.234. Section 440.105(7), |
OF PHYSICIAN OR HOSPITAL |
|
|
|
|||||||||||||||
F.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I have reviewed, understand and acknowledge the above statement. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
__________________________________________________________________ |
|
_______________________________________________ |
|
|
|
|
|
|
|||||||||||
|
EMPLOYEE SIGNATURE (If available to sign) |
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|||
__________________________________________________________________ |
|
_______________________________________________ |
|
|
|
|
|
|
|||||||||||
|
|
EMPLOYER SIGNATURE |
|
|
|
|
|
DATE |
|
|
|
|
AUTHORIZED BY EMPLOYER |
YES |
NO |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
1(a) |
Denied Case - |
|
|
|
2. Medical Only which became Lost Time Case (Complete all required information in #3) |
|
|||||||||||||
1(b) |
Indemnity Only Denied Case - |
|
Employee’s 8TH Day of Disability |
_________ / _________ / _________ |
|
||||||||||||||
|
|
|
|
|
|
|
|
Entity’s Knowledge of 8TH Day of Disability _________ /_________ / _________ |
|
|
|||||||||
3. Lost Time Case - 1st day of disability _________ / _________ / _________ |
Full Salary in lieu of comp? |
YES |
Full Salary End Date ________/ ________ / ________ |
|
|||||||||||||||
Date First Payment Mailed _________ / _________ / _________ |
AWW ____________________________ |
Comp Rate ____________________________ |
|
|
|||||||||||||||
|
T.T. |
T.T. - 80% |
T.P. |
I.B. |
P.T. |
DEATH |
|
SETTLEMENT ONLY |
|
|
|
|
|||||||
Penalty Amount Paid in 1st Payment $___________ |
Interest Amount Paid in 1st Payment $__________ |
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
REMARKS: |
|
|
|
|
|
|
|
|
|
|
INSURER NAME |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
INSURER CODE # |
|
EMPLOYEE'S CLASS CODE |
|
|
EMPLOYER'S NAICS CODE |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
SERVICE CO/TPA CODE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
The collection of the social security number on this form is specifically authorized by Section 440.185(2), Florida Statutes. The social security number will be used as a unique identifier in Division of Workers' Compensation database systems for individuals who have claimed benefits under Chapter 440, Florida Statutes. It will also be used to identify information and documents in those database systems regarding individuals who have claimed benefits under Chapter 440, Florida Statutes, for internal agency tracking purposes and for purposes of responding to both public records requests and subpoenas that require production of specified documents. The social security number may also be used for any other purpose specifically required or authorized by state or federal law.
Document Specifics
| Fact Name | Detail |
|---|---|
| Document Title | FIRST REPORT OF INJURY OR ILLNESS |
| Authorizing Agency | FLORIDA DEPARTMENT OF FINANCIAL SERVICES DIVISION OF WORKERS' COMPENSATION |
| Assistance Contact Information | For assistance call 1-800-342-1741 or contact your local EAO Office |
| Reporting Requirement for Deaths | Report all deaths within 24 hours to 1-800-219-8953 or (850) 922-8953 |
| Governing Law | Section 440.105(7), F.S. for insurance fraud and Section 440.185(2), Florida Statutes for social security number collection and use |
| Form Identification | DFS-F2-DWC-1 (03/2009) Rule 69L-3.025, F.A.C. |
Guide to Writing First Report Dfs F2 Dwc 1
Filling out the First Report of Injury or Illness (Form DFS-F2-DWC-1) is a crucial step for reporting workplace injuries or illnesses in Florida. This document, required by the Florida Department of Financial Services Division of Workers' Compensation, ensures timely communication between employers, employees, and the Division. It's important to fill out this form accurately to avoid delays in processing workers' compensation claims. Below are straightforward steps to complete the form.
- Start by entering the date the report is being sent to the division in the "SENT TO DIVISION DATE" section.
- Complete the "EMPLOYEE INFORMATION" section with the employee's full name, social security number, date of the accident, time of the accident (AM/PM), home address, telephone number, occupation, injury/illness details, part of the body affected, date of birth, and sex.
- Under "EMPLOYER INFORMATION," fill in the federal ID number (FEIN), the date the injury or illness was first reported, company name, doing business as (DBA) name if applicable, nature of the business, policy/member number, company address, telephone number, date employed, and if you'll continue to pay wages instead of workers' compensation.
- Provide details about the accident's location, the employee's return to work status, the last date wages will be paid instead of workers' comp (if applicable), date of death (if applicable), rate of pay, place of accident, and whether you agree with the description of the accident.
- Include the name, address, and telephone number of the physician or hospital that attended to the employee.
- If the employee is available and agrees with the information provided, have them sign the form along with the date.
- The employer or authorized person should sign the form, indicating whether the signing individual is authorized by the employer.
- In the "CLAIMS-HANDLING ENTITY INFORMATION" section, check the appropriate boxes based on the case type and complete all required fields, including the employee’s 8th day of disability, entity’s knowledge of 8th day of disability, lost time case details, full salary in lieu of comp, date first payment mailed, average weekly wage, compensation rate, and any penalties or interest paid in the first payment.
- Finalize the form by filling out the "REMARKS" section with any additional notes, the insurer and claims-handling entity's name, address, and telephone, along with several codes related to the employee, employer, and the entity handling the claim.
After completing the form, review all information for accuracy to ensure a smooth submission process. Submit the form following the directions provided by the Florida Department of Financial Services Division of Workers' Compensation. This might involve sending it through mail, email, or an online submission portal, depending on the required or preferred method.
Understanding First Report Dfs F2 Dwc 1
-
What is the purpose of the First Report of Injury or Illness (Form DFS-F2-DWC-1) and who should use it?
This form is specifically designed for reporting workplace injuries or illnesses in the state of Florida. It serves as the initial notification to the Florida Department of Financial Services, Division of Workers' Compensation, about an employee's work-related injury or illness. Employers or their claims-handling entities must complete and submit this form to comply with state regulations and ensure the injured employee receives the appropriate workers' compensation benefits.
-
How soon after an incident must the First Report of Injury or Illness be filed?
It's crucial for employers to submit this form as promptly as possible. The state of Florida requires that all workplace deaths are reported within 24 hours. For non-fatal injuries or illnesses, employers should aim to file the report as soon as they are informed of the incident to expedite the claims process and support timely medical care for the employee.
-
What information is required on the form?
The form requires detailed information about the injured or ill employee, including their name, social security number, date of birth, occupation, and a description of the injury or illness and how it occurred. It also asks for employer information, details of the incident (such as the time, date, and place of accident), and information about the treating physician or hospital. Validating this information with signatures from both the employee (if available) and the employer is also required.
-
Can wages be paid instead of workers' compensation? How should this be reported on the form?
Yes, employers have the option to continue paying wages in lieu of workers' compensation benefits. This choice must be clearly indicated on the form, including whether wages will continue to be paid, the last day wages were paid in lieu of workers' comp, and if so, the date wages will cease. This information helps ensure clear communication and proper handling of the employee's compensation benefits.
-
What happens if the employer disagrees with the employee’s description of the accident?
The form provides a section for employers to indicate whether they agree with the employee's description of the accident. If there's a disagreement, employers should still submit the report promptly and may provide additional remarks or documentation to the Division of Workers' Compensation to elaborate on their perspective. It’s important to handle disagreements professionally and comply with all reporting requirements to ensure the issue is resolved fairly.
-
Where should the First Report of Injury or Illness be sent after completion?
After filling out the form, it should be sent to the Division of Workers' Compensation through the Florida Department of Financial Services. The form’s detailed submission instructions, including specific addresses or electronic submission guidelines, can be obtained from the Division’s website or by contacting the Florida Department of Financial Services directly for assistance.
-
What penalties exist for submitting false or misleading information on this form?
It's a serious offense to knowingly provide false or misleading information on the First Report of Injury or Illness. Such actions can be considered insurance fraud, punishable under Section 817.234, Florida Statutes. Penalties may include fines, restitution, and even criminal charges. It underscores the importance of ensuring all information provided on the form is accurate and truthful.
-
Who can assist with completing the First Report of Injury or Illness?
Employers uncertain about how to correctly complete the form can seek assistance from the Division of Workers' Compensation. Support is available via a toll-free helpline or by contacting a local Employee Assistance Office (EAO). These resources can provide guidance and help clarify any questions regarding the proper filing of the report.
-
Why is the employee’s social security number required on the form?
The collection of social security numbers on the First Report of Injury or Illness is authorized by Section 440.185(2), Florida Statutes. The primary purpose is to use the social security number as a unique identifier in the Division of Workers' Compensation database systems. It facilitates the tracking of individuals who have claimed benefits and supports the identification of documents and information within these systems. This measure also aids in complying with public records requests and subpoenas requiring document production.
Common mistakes
Filling out the First Report of Injury or Illness (DFS-F2-DWC-1) is a critical step in initiating a workers' compensation claim in Florida. However, errors in the process can delay or negatively impact a claim. Here are common mistakes to avoid:
Incorrect or Incomplete Employee Information: It is vital to provide full and accurate details, including the correct spelling of the employee's name, their social security number, date of birth, and precise contact information. Missing or incorrect information can lead to processing delays.
Failing to Accurately Describe the Accident: The employee's description of the accident and cause of injury needs to be detailed. Including how, when, and where the incident occurred offers clarity and supports the claim's verification process.
Incorrect Date and Time of Accident: It's essential to report the exact date and time of the accident. This information should be consistent across all documentation related to the claim.
Misidentifying the Location of Accident: The specific place where the injury occurred, including the street, city, state, and zip code, needs to be accurately documented. An unclear or wrong location can complicate the verification process.
Not Reporting the Injury to the Employer Promptly: The date the injury was first reported to the employer should be clearly documented. Delays in reporting can affect the legitimacy and processing of the claim.
Omitting Information on Wages and Employment: Details such as the rate of pay, whether wages will continue to be paid in lieu of workers' compensation, and employment status at the time of injury are critical for determining compensation amounts.
Incorrect Employer or Policy Information: Providing accurate details about the employer, including the federal I.D. number, nature of business, and policy/member number, is essential for processing the claim.
Neglecting to Document Agreement on Accident Description: Both the employee and employer must indicate whether they agree with the description of the accident. Failing to document this can lead to disputes or delays in claim processing.
Avoiding these mistakes helps ensure that the claims process moves smoothly and efficiently. Attention to detail and accurate reporting supports a clear understanding of the circumstances surrounding the injury or illness, assisting all parties involved in the workers' compensation system.
Documents used along the form
When it comes to navigating the world of workers' compensation, particularly in Florida, the First Report of Injury or Illness form, known as the DFS-F2-DWC-1, is a critical document that businesses must familiarize themselves with. It serves as the initial report filed by an employer to notify the Florida Department of Financial Services and Division of Workers' Compensation of an employee’s work-related injury or illness. However, this form is often just the beginning of a documentation journey. Below is a list of other forms and documents that are frequently used alongside the DFS-F2-DWC-1 form, each serving its unique purpose in the course of a workers' compensation claim.
- DWC-12: Notice of Denial - This form is utilized by employers or their insurance to deny a workers' compensation claim. It officially informs the injured worker that their claim won't be compensated under workers' compensation insurance, detailing the reasons for denial.
- DWC-3: Employee Earnings Report - Submitted by the injured employee, this form outlines the wages earned before and after the injury, providing a basis for determining compensation benefits.
- DWC-4: Doctor's Report - Completed by the treating physician, it provides detailed medical information about the employee's injury or illness, prognosis, and work status, directly impacting benefit determinations.
- WCC-1: Employee Claim Form - An injured worker uses this form to formally file a claim for workers' compensation benefits, describing the nature and circumstances of the injury or illness.
- DWC-25: Work Status Report - This essential form is updated regularly by the treating healthcare provider to report the employee's current work capabilities, which helps in determining when and in what capacity the employee can return to work.
- DWC-60: Request for Social Security Disability Benefit Information - Often submitted by the claims-handling entity, this form requests information about an injured worker's Social Security Disability Insurance (SSDI) benefits, which can affect workers' compensation benefits.
- DFS-F4-1590: Division of Workers' Compensation Compliance Proof of Coverage Database Search Request - Used to verify an employer’s workers' compensation insurance coverage, which is critical in the event of a dispute or claim against a purportedly uninsured employer.
Together, these forms create a comprehensive landscape that ensures the accurate reporting, treatment, and compensation of work-related injuries and illnesses. For employers, understanding these documents is key to managing their responsibilities under Florida law. And for employees, being informed about these additional forms can facilitate a smoother, more transparent claim process, leading to better outcomes for all parties involved.
Similar forms
The OSHA Form 300, also known as the Log of Work-Related Injuries and Illnesses, bears similarity to the First Report of Injury or Illness (First Report DFS F2 DWC 1). Both forms are essential for documenting workplace injuries or illnesses. The OSHA Form 300 serves a broader function by providing a detailed log of all work-related injuries and illnesses within a specific timeframe, whereas the First Report focuses on documenting a single incident. Each form plays a critical role in workplace safety and health compliance, helping to identify patterns of injuries and areas for improvement.
The Employer's First Report of Injury or Illness, which varies by state, is another document akin to Florida's First Report DFS F2 DWC 1 form. This report is the initial notification to state workers' compensation boards about an employee’s work-related injury or illness, similar to the First Report’s role in Florida. While specifics of the form may differ across jurisdictions, the primary purpose remains consistent: to kickstart the process of a workers' compensation claim, ensuring that employees receive appropriate medical care and compensation for workplace injuries or illnesses.
The CA-1 Federal Employee's Notice of Traumatic Injury and Claim for Continuation of Pay/Compensation is a form used by federal employees, drawing parallels to the Florida-specific First Report. Though this form is specifically for federal employees and the First Report for those covered under Florida’s jurisdiction, both documents serve to formally report an injury or illness. They document essential details about the incident, helping to ensure the injured party receives timely medical attention and compensation benefits.
The DWC 1 Form, known as the Workers' Compensation Claim Form, is particularly similar to the First Report DFS F2 DWC 1 in its objective and use within workers' compensation systems, albeit California’s version. When an employee gets injured or becomes ill due to work, filling out the DWC 1 Form is a crucial first step in claiming workers' compensation benefits in California. This process mirrors the function of Florida’s First Report, even though each form adheres to the regulations and requirements of its respective state.
The Employee's Report of Injury Form is another document related to the First Report of Injury or Illness. While the name and specifics can vary depending on the employer or state, the primary purpose is for employees to report any workplace injuries or illnesses to their employer. This serves as an internal record for the employer and can be a precursor to filling out state-specific workers' compensation claim forms, such as the First Report in Florida. Both types of documents are crucial for maintaining an official record of the incident and further processing the employee's claim for benefits.
Dos and Don'ts
When you're filling out the First Report of Injury or Illness (DFS-F2-DWC-1) for the Florida Department of Financial Services Division of Workers' Compensation, it's critical to pay close attention to details to ensure the process is handled accurately and efficiently. Here are several dos and don'ts to keep in mind:
Dos:- Do thoroughly review the entire form first before starting to fill it out. This will give you a clear understanding of what information is required.
- Do use black or blue ink and print clearly if filling out the form by hand to make sure all information is legible.
- Do provide accurate and detailed information about the accident, including the cause of the injury and the specific part of the body affected.
- Do report all fatalities within 24 hours as required by the instructions at the top of the form.
- Do double-check the social security number and employee information to ensure accuracy. This is critical for tracking and verification purposes.
- Do include complete employer and insurance information, including policy numbers and the claims-handling entity details.
- Do sign the form and make sure it's also signed by the employer, as these signatures are crucial for the form's validity.
- Don't leave any required fields blank. If a section does not apply, it's better to mark it as "N/A" (Not Applicable) rather than leaving it empty.
- Don't forget to include the date of accident and the exact time it occurred, as this information is crucial for the claim.
- Don't provide vague descriptions of the accident or injury. Be as specific as possible to avoid delays in processing the claim.
- Don't underestimate the importance of the accident location details. Include the complete address where the injury occurred.
- Don't ignore the section on the employee's description of the accident. This narrative is vital for understanding how the injury happened.
- Don't submit the form without reviewing it for mistakes or missing information. Errors can complicate and slow down the claims process.
- Don't forget to call the assistance numbers provided at the top of the form if you have any questions or require help filling it out.
Misconceptions
Understanding the complexities of workers' compensation forms can be challenging, and the First Report of Injury or Illness (Form DFS-F2-DWC-1) is no exception. This form plays a crucial role within the Florida Department of Financial Services, Division of Workers' Compensation process. However, misconceptions about its use and requirements can lead to confusion. Here are six common misconceptions about this form:
- It's only for reporting deaths. While the form requires that all deaths be reported within 24 hours, it's actually used for reporting any workplace injury or illness, not just fatalities. Its primary purpose is to initiate a workers' compensation claim process for injured employees.
- Only the employee needs to sign the form. In reality, both the employee (if able to sign) and the employer need to provide signatures. This ensures that both parties acknowledge the reported incident and the information submitted is accurate to the best of their knowledge.
- Employers have unlimited time to report an incident. Timeliness is critical in workers' compensation cases. Florida statutes require that this form be submitted promptly after an employer becomes aware of an employee's injury or illness related to work. Delay in reporting can lead to penalties and affect the processing of the claim.
- The form is complicated and requires legal knowledge to complete. While it's comprehensive, the form is designed to be filled out by employers without needing specialized legal knowledge. It asks for factual information about the employee, the injury or illness, and the circumstances surrounding the incident.
- You need to submit this form for minor injuries that don't require medical attention. The necessity to report an injury depends on its severity and whether it leads to medical treatment or missed workdays. However, it's often wise to report any workplace injury, no matter how minor it seems initially, to avoid any potential complications later on.
- Submitting this form is the responsibility of the employee. It is actually the employer’s responsibility to complete and submit the First Report of Injury or Illness. While employees should notify their employer about any workplace injury or illness, the formal reporting process through this form falls on the employer.
Correcting these misconceptions is crucial for ensuring that the workers' compensation process is navigated efficiently and effectively. Both employers and employees must understand their rights and responsibilities clearly. Accurate completion and timely submission of the First Report of Injury or Illness form not only comply with Florida's legal requirements but also facilitate the injured employee's access to benefits and support during recovery.
Key takeaways
Filling out and using the First Report of Injury or Illness (Form DFS-F2-DWC-1) is critical in the process of reporting a workplace injury or illness in Florida. Here are some key takeaways to ensure this form is correctly completed and utilized:
- Timeliness is crucial: All deaths must be reported within 24 hours. This prompt reporting ensures that necessary steps are taken without delay.
- Accuracy matters: When filling out the form, it's important to ensure that all the information provided is accurate and complete. This includes the employee's personal information, the detailed description of the accident (including the cause of injury), and the employer's information.
- Use of social security number: The collection of the social security number is specifically authorized and used as a unique identifier in the Division of Workers' Compensation database systems. It helps in tracking the claim efficiently.
- Signature requirement: Both the employee (if available to sign) and the employer must sign the form. Their signatures acknowledge the information provided and confirm its accuracy.
- Reporting the details of the accident: Agreeing with the description of the accident is essential. It is necessary for the employer to verify and confirm that the details provided by the employee match their understanding of the incident.
- Handling and submission: Once completed, the form should be sent to the Division of Workers' Compensation. Keeping a copy for records is also advisable. Knowing where and how to submit the form is important for a smooth processing of the claim.
Understanding these key aspects can help in the effective management of workers' compensation claims in Florida, ensuring that employees receive the appropriate care and support following a workplace injury or illness.
Popular PDF Documents
Wv State Tax Forms - The form reiterates the importance of meeting minimum payment thresholds to avoid penalties.
What Is Power of Attorney California - Hand over your tax responsibilities to a designated agent, ensuring your affairs are handled diligently and lawfully.